You might also like
- Pediatric Soap NoteDocument4 pagesPediatric Soap NoteAfinaMuthi50% (2)
- Interpretive standards and control zone diameters for antimicrobial susceptibility testingDocument16 pagesInterpretive standards and control zone diameters for antimicrobial susceptibility testingGeoemilia180% (5)
- Antibiotics Summary - Flattened PDFDocument3 pagesAntibiotics Summary - Flattened PDFmicheal1960100% (6)
- Tonsillitis Pathophysiology, Symptoms and TreatmentDocument8 pagesTonsillitis Pathophysiology, Symptoms and TreatmentApril Grace LoredoNo ratings yet
- Pneumonia Case StudyDocument33 pagesPneumonia Case StudyArceo AbiGail100% (3)
- Case Presentation - Acute Otits MediaDocument31 pagesCase Presentation - Acute Otits MediaJean nicole Garibay0% (1)
- Case StudyDocument21 pagesCase StudyLuige AvilaNo ratings yet
- 5 - Antibiotics 2018Document11 pages5 - Antibiotics 2018nae100% (3)
- IMCI AnswerDocument8 pagesIMCI AnswerQuia Benjch Uayan100% (3)
- Antibiotics Study Guide For NursesDocument3 pagesAntibiotics Study Guide For NursesLauren Trotman100% (7)
- Cardiac Case Study NDDocument11 pagesCardiac Case Study NDapi-313165458No ratings yet
- Case Study Tonsil It IsDocument16 pagesCase Study Tonsil It IsMuhammad FarhanNo ratings yet
- Predisposing and Precipitating Factors of TuberculosisDocument3 pagesPredisposing and Precipitating Factors of Tuberculosisemely p. tangoNo ratings yet
- Ineffective Breathing Pattern Related To Acute Pain As Evidence by Increased RespirationDocument6 pagesIneffective Breathing Pattern Related To Acute Pain As Evidence by Increased RespirationCamille T. SanchezNo ratings yet
- Nursing Care of Bronchial AsthmaDocument16 pagesNursing Care of Bronchial AsthmaIntan RahmiNo ratings yet
- Case Studies - Tetralogy of FallotDocument16 pagesCase Studies - Tetralogy of FallotKunwar Sidharth SaurabhNo ratings yet
- TonsillitisDocument10 pagesTonsillitisjessyNo ratings yet
- How Phototherapy WorksDocument4 pagesHow Phototherapy WorksmaramNo ratings yet
- Case Study,,,,,,pneumoniaDocument52 pagesCase Study,,,,,,pneumoniaJaillah Reigne Cura0% (1)
- Case Presentation 3 DR Oscar Laryngitis TBDocument33 pagesCase Presentation 3 DR Oscar Laryngitis TBmarajuu50% (2)
- Case Study On LeukemiaDocument33 pagesCase Study On LeukemiaBhupesh PatidarNo ratings yet
- Family Case Study For HydrocephalusDocument9 pagesFamily Case Study For HydrocephalusjaegergranNo ratings yet
- Hydrocephalus Nursing CareDocument27 pagesHydrocephalus Nursing CareyounggirldavidNo ratings yet
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangNo ratings yet
- Case Presentation About Hypertension Stage 2-BeluanDocument36 pagesCase Presentation About Hypertension Stage 2-BeluanKeepItSecretNo ratings yet
- PHARYNGITISDocument8 pagesPHARYNGITISWàrìs Ràfìqùé ßàlòçhNo ratings yet
- CP On AGEDocument31 pagesCP On AGELeah CaressaNo ratings yet
- BSC Nursing Guide: Tonsillitis and AdenoiditisDocument41 pagesBSC Nursing Guide: Tonsillitis and AdenoiditisYAMINIPRIYANNo ratings yet
- Tuberculosis and Nephrotic Syndrome in a ChildDocument34 pagesTuberculosis and Nephrotic Syndrome in a ChildAldo YustiantoNo ratings yet
- Laryngitis and Upper Airway ObstructionDocument9 pagesLaryngitis and Upper Airway Obstructionjonna casumpangNo ratings yet
- EpistaxisDocument33 pagesEpistaxispaulyn ramosNo ratings yet
- Etiology of TonsillitisDocument15 pagesEtiology of TonsillitisRendy Candra100% (1)
- CHN FinalsDocument15 pagesCHN FinalsLyndon SayongNo ratings yet
- Community-Acquired Pneumonia DiagnosisDocument102 pagesCommunity-Acquired Pneumonia DiagnosisJay Kumar100% (1)
- Assessment Nursing Diagnosis Planning Interventions EvaluationsDocument4 pagesAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanNo ratings yet
- Otitis MediaDocument39 pagesOtitis MediaGilian Dacanay100% (4)
- Drug-Study-Ncp-And-Fdar - Sir WencyDocument21 pagesDrug-Study-Ncp-And-Fdar - Sir WencyBiway RegalaNo ratings yet
- Lesson Plan On CholelithiasisDocument12 pagesLesson Plan On CholelithiasisKaka SalvatoreNo ratings yet
- QuizDocument16 pagesQuizDawn MarcoNo ratings yet
- CroupDocument20 pagesCroupFariezuan HamidNo ratings yet
- Iloilo Doctors' College Case Study on PneumoniaDocument38 pagesIloilo Doctors' College Case Study on PneumoniaLuna JadeNo ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- Case Study-Chronic TonsillitisDocument7 pagesCase Study-Chronic TonsillitisJonalyn TumanguilNo ratings yet
- BronchitisDocument6 pagesBronchitisNader Smadi100% (1)
- Glaucoma: DefinitionDocument5 pagesGlaucoma: DefinitionDani PhilipNo ratings yet
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- TIA Case StudyDocument3 pagesTIA Case StudySanny Ramos100% (1)
- Angina PectorisDocument17 pagesAngina PectorisRacel HernandezNo ratings yet
- Case Report - Deep Vein ThrombosisDocument12 pagesCase Report - Deep Vein ThrombosisAndi Meidin AnugerahNo ratings yet
- MorphineDocument3 pagesMorphineAizat KamalNo ratings yet
- Case PresentationDocument46 pagesCase PresentationAileen DometitaNo ratings yet
- Hydrocephalus 9Document9 pagesHydrocephalus 9Shesly PhilominaNo ratings yet
- Modified CaseDocument22 pagesModified CaseAli HawamdeNo ratings yet
- Case Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andDocument38 pagesCase Presentation OF Acute Tonsillitis: Nueva Ecija University of Science andBeverly DatuNo ratings yet
- Case Study 1 FinalDocument28 pagesCase Study 1 Finalapi-3905968320% (1)
- Brain Tumor DiagnosisDocument65 pagesBrain Tumor DiagnosisMichelle Vera GabunNo ratings yet
- Meconium Aspiration Syndrome: Causes, Symptoms and TreatmentDocument13 pagesMeconium Aspiration Syndrome: Causes, Symptoms and TreatmentSANANo ratings yet
- Case Study On Pulmonary EmbolismDocument12 pagesCase Study On Pulmonary EmbolismJobelle Acena100% (2)
- Hypovolemic Shock 09Document58 pagesHypovolemic Shock 09Joanne Bernadette Aguilar100% (2)
- PP's Bronchitis CaseDocument28 pagesPP's Bronchitis Caseroselyn valdezNo ratings yet
- NURSING CARE ON CLIENTS WITH DIARRHEADocument30 pagesNURSING CARE ON CLIENTS WITH DIARRHEAyustiNo ratings yet
- NCP TBDocument7 pagesNCP TBLorraine CilloNo ratings yet
- Case Report Chronic OsteomyelitisDocument34 pagesCase Report Chronic OsteomyelitisNardine Roslan100% (1)
- Articles English TyphoidDocument13 pagesArticles English TyphoidSiDewiAjja100% (1)
- Mengapa Pasien Merasakan Seperti Sensasi Terbakar Dan Nyeri Telan Pada Tenggorokan?Document19 pagesMengapa Pasien Merasakan Seperti Sensasi Terbakar Dan Nyeri Telan Pada Tenggorokan?Nasia GustinaNo ratings yet
- Significance of Study on Elderly Functional HealthDocument2 pagesSignificance of Study on Elderly Functional HealthkdfhjfhfNo ratings yet
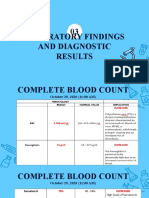
- Laboratory Findings and Diagnostic Results 03Document4 pagesLaboratory Findings and Diagnostic Results 03kdfhjfhfNo ratings yet
- Community Healthy NursingDocument1 pageCommunity Healthy NursingkdfhjfhfNo ratings yet
- Death Voice OverDocument3 pagesDeath Voice OverkdfhjfhfNo ratings yet
- Synchronous Class Schedule For: Time 1 and 3 Week of The Month 2 and 4 Week of The Month Wednesday Friday Wednesday FridayDocument1 pageSynchronous Class Schedule For: Time 1 and 3 Week of The Month 2 and 4 Week of The Month Wednesday Friday Wednesday FridaykdfhjfhfNo ratings yet
- RRL LocalinternationalDocument11 pagesRRL LocalinternationalkdfhjfhfNo ratings yet
- Name: Celajes, Ma. Lourdes Ann D. Group: D: Rarely (1) Sometimes (2) Usually (3) Almost AlwaysDocument3 pagesName: Celajes, Ma. Lourdes Ann D. Group: D: Rarely (1) Sometimes (2) Usually (3) Almost AlwayskdfhjfhfNo ratings yet
- Hepatobiliary Ultrasound Finds Enlarged Liver and SpleenDocument7 pagesHepatobiliary Ultrasound Finds Enlarged Liver and SpleenkdfhjfhfNo ratings yet
- Liao E. Sci Food and Agriculture QuizDocument5 pagesLiao E. Sci Food and Agriculture QuizkdfhjfhfNo ratings yet
- Jean Watson Cerr0Document1 pageJean Watson Cerr0kdfhjfhfNo ratings yet
- Name Name Name: AnswerDocument2 pagesName Name Name: AnswerkdfhjfhfNo ratings yet
- B. 89101112 Malignancy EmaDocument13 pagesB. 89101112 Malignancy EmakdfhjfhfNo ratings yet
- Cinco John Joshua EnviSci Activity Health and Energy UseDocument1 pageCinco John Joshua EnviSci Activity Health and Energy UsekdfhjfhfNo ratings yet
- ACTH Test GuideDocument11 pagesACTH Test GuidekdfhjfhfNo ratings yet
- The Type of Cancer SuspectedDocument20 pagesThe Type of Cancer SuspectedkdfhjfhfNo ratings yet
- Diagnostic Test Normal Findins Description Purpose Indication Procedure Nursing Implications Magnetic Resonance ImagingDocument5 pagesDiagnostic Test Normal Findins Description Purpose Indication Procedure Nursing Implications Magnetic Resonance ImagingkdfhjfhfNo ratings yet
- Laboratory/Diagnostic Exams: WORKSHEET ON Endocrine System DisordersDocument153 pagesLaboratory/Diagnostic Exams: WORKSHEET ON Endocrine System DisorderskdfhjfhfNo ratings yet
- Case Scenario 5 NCPDocument10 pagesCase Scenario 5 NCPkdfhjfhfNo ratings yet
- Cesar - EvaluationDocument2 pagesCesar - EvaluationkdfhjfhfNo ratings yet
- Tumor Marker Test A. Prostate Specific Antigen (Psa) TestDocument25 pagesTumor Marker Test A. Prostate Specific Antigen (Psa) TestkdfhjfhfNo ratings yet
- Normal Findings and MeaningDocument11 pagesNormal Findings and MeaningkdfhjfhfNo ratings yet
- Laboratory/Diagnostic Exams: WORKSHEET ON Endocrine System DisordersDocument145 pagesLaboratory/Diagnostic Exams: WORKSHEET ON Endocrine System DisorderskdfhjfhfNo ratings yet
- Cesar, Katyana Antoine - Common Laboratory and Diagnostics Procedures Used in Gi Disorders (Rle Worksheet No. 3)Document30 pagesCesar, Katyana Antoine - Common Laboratory and Diagnostics Procedures Used in Gi Disorders (Rle Worksheet No. 3)kdfhjfhfNo ratings yet
- Cesar - Cardio & HemaDocument77 pagesCesar - Cardio & HemakdfhjfhfNo ratings yet
- 4 Collab Ws VH KasDocument2 pages4 Collab Ws VH KaskdfhjfhfNo ratings yet
- Case Scenario 2 NCP RevisedDocument5 pagesCase Scenario 2 NCP RevisedkdfhjfhfNo ratings yet
- Cesar - Evaluation - ImciDocument3 pagesCesar - Evaluation - ImcikdfhjfhfNo ratings yet
- Cesar, Katyana Antoine - Vision & Hearing LecDocument17 pagesCesar, Katyana Antoine - Vision & Hearing LeckdfhjfhfNo ratings yet
- WORKSHEET IN NCM 109.vision& HearingDocument2 pagesWORKSHEET IN NCM 109.vision& HearingkdfhjfhfNo ratings yet
- PenicillinsDocument7 pagesPenicillinsZain BaderNo ratings yet
- Penicillins - KatzungDocument6 pagesPenicillins - KatzungKarl CNo ratings yet
- Peta Kuman 2022Document3 pagesPeta Kuman 2022Musyafa'atun AnitaNo ratings yet
- NCLEX REVIEW AntibioticsDocument7 pagesNCLEX REVIEW Antibioticsneonstar100% (1)
- Introduction to commonly used antibioticsDocument2 pagesIntroduction to commonly used antibioticsAmir AmirulNo ratings yet
- Journal Reading Impetigo BulosaDocument16 pagesJournal Reading Impetigo BulosaFery LamperoughNo ratings yet
- Drug Index Updated2Document113 pagesDrug Index Updated2tam meiNo ratings yet
- MID 3 PHARMA Chemotherapeutic AgentsDocument85 pagesMID 3 PHARMA Chemotherapeutic AgentsMariah Angela PinedaNo ratings yet
- International Medical Guide For Ships (Quantification Addendum) Third EditionDocument58 pagesInternational Medical Guide For Ships (Quantification Addendum) Third EditionΔΗΜΗΤΡΗΣΧΑΛΑΤΣΗΣ100% (1)
- Splenectomy: DisclaimerDocument5 pagesSplenectomy: DisclaimerMimi FatinNo ratings yet
- Dedicated to Safe Your LifeDocument120 pagesDedicated to Safe Your LifeABILAH SALUMNo ratings yet
- AdventDocument17 pagesAdventnishant_singh_80100% (1)
- PA ToolDocument42 pagesPA ToolShara Lailanie A. AzisNo ratings yet
- The GP Note 2020Document306 pagesThe GP Note 2020firdauseahNo ratings yet
- Papp Perspective: Philippine Academy of Pediatric Pulmonologists, IncDocument54 pagesPapp Perspective: Philippine Academy of Pediatric Pulmonologists, IncMarko Parungo100% (1)
- Torvastatin Side Effects: Allergic Reaction To Atorvastatin: Hives DifficultyDocument11 pagesTorvastatin Side Effects: Allergic Reaction To Atorvastatin: Hives Difficulty'Prasada WedatamaNo ratings yet
- Hi-Pro Veterinary Compendium 03 21 2017 PDFDocument252 pagesHi-Pro Veterinary Compendium 03 21 2017 PDFFranklin MartinezNo ratings yet
- Drug ListDocument104 pagesDrug Listخانه پزشکNo ratings yet
- Evaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalDocument6 pagesEvaluation of Prescribing Patterns of Antibiotics in General Medicine Ward in A Tertiary Care HospitalEditor IJTSRDNo ratings yet
- GNR Bacteremia De-Escalation Guide Final PDFDocument2 pagesGNR Bacteremia De-Escalation Guide Final PDFAbu Hammoud AlyazeediNo ratings yet
- OAU Antibiotic Class DefinitionsDocument2 pagesOAU Antibiotic Class DefinitionsHenan Educational ServicesNo ratings yet
- Antibiotics ChartDocument10 pagesAntibiotics ChartTrina Si100% (6)
- Ceiling-Price-List-F 30 Sep 2020Document21 pagesCeiling-Price-List-F 30 Sep 2020nagashayana gNo ratings yet
- Viii. Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument8 pagesViii. Nursing Care Plan Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationronronNo ratings yet