You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Fat Loss For LifeDocument42 pagesFat Loss For LifeDjuli Ona83% (12)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cerebrovascular DiseaseDocument54 pagesCerebrovascular Diseaselisaagustina100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Alpha Male State of Mind PDFDocument12 pagesAlpha Male State of Mind PDFRideIT0% (1)
- A Collection of Short Stories (Volume 2)Document109 pagesA Collection of Short Stories (Volume 2)Christopher HodgeNo ratings yet
- Surya KriyaDocument9 pagesSurya KriyaAnonymous VXIcsYNo ratings yet
- Nursing AssesmentDocument39 pagesNursing AssesmentRed Jimeno100% (1)
- MCQ RespiratoryDocument6 pagesMCQ Respiratorynurulhudaabdulmuiez100% (2)
- Pharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeDocument49 pagesPharmacology: Nepthali Christuar Aldueza, R.N. Calamba Doctors CollegeArielle Joy Atienza100% (1)
- Metabolic Basis of Human DiseaseDocument25 pagesMetabolic Basis of Human DiseaseDr Science YNo ratings yet
- Reading TP 5Document5 pagesReading TP 5Nadia ReineroNo ratings yet
- Left-Sided Heart FailureDocument3 pagesLeft-Sided Heart FailureKhalid Mahmud ArifinNo ratings yet
- Ks4 Characteristics and Classification of Living OrganismsDocument42 pagesKs4 Characteristics and Classification of Living OrganismsDaniella AjalaNo ratings yet
- Rate Coding and The Control of Muscle ForceDocument12 pagesRate Coding and The Control of Muscle ForceMirna Liliana Carmona GarciaNo ratings yet
- Module in P.E. and Health Shs - Grade 11 Alupay SHS First QuarterDocument5 pagesModule in P.E. and Health Shs - Grade 11 Alupay SHS First QuarterZsazha Necolet Gonzaga - Cabrera0% (1)
- Transport Mechanism Lecture BestDocument9 pagesTransport Mechanism Lecture Bestelyza gwenNo ratings yet
- FrogDocument65 pagesFrognarayan sahNo ratings yet
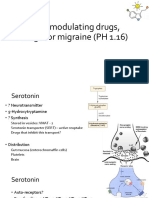
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Document13 pages5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNo ratings yet
- Final U6 p2 2010Document6 pagesFinal U6 p2 2010Cindy ChuahNo ratings yet
- Cardiac L3Document18 pagesCardiac L3Qutaybah JahmanyNo ratings yet
- BSC 250 Chapter 3 Blank NotesDocument10 pagesBSC 250 Chapter 3 Blank NotessarahreyNo ratings yet
- Terapi Cairan Resusitasi: DR Arief Munandar, Span, Kic Bagian Anestesi - Icu Rsud BrebesDocument34 pagesTerapi Cairan Resusitasi: DR Arief Munandar, Span, Kic Bagian Anestesi - Icu Rsud BrebesWistha MiyakiNo ratings yet
- BloodDocument11 pagesBloodMohamad YusriNo ratings yet
- Appearance of Anatomic Structures On Panoramic ImageDocument18 pagesAppearance of Anatomic Structures On Panoramic ImageRishabh Madhu SharanNo ratings yet
- Full Download Human Anatomy and Physiology Marieb 8th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Human Anatomy and Physiology Marieb 8th Edition Test Bank PDF Full Chapterephod.pyurianheta100% (15)
- Parkinsonism and Related Disorders: David A. Low, Ekawat Vichayanrat, Valeria Iodice, Christopher J. MathiasDocument5 pagesParkinsonism and Related Disorders: David A. Low, Ekawat Vichayanrat, Valeria Iodice, Christopher J. MathiasRafael Yokoyama FecchioNo ratings yet
- Lymphatic Drainage of The ThoraxDocument1 pageLymphatic Drainage of The ThoraxYusri ArifNo ratings yet
- Massage Technique PetrissageDocument5 pagesMassage Technique PetrissageNelia Banez PatalayNo ratings yet
- Choice of Anesthetic Technique MillerDocument10 pagesChoice of Anesthetic Technique MillersffNo ratings yet
- Nursing Care Plan HF FinalDocument10 pagesNursing Care Plan HF FinalCristina L. JaysonNo ratings yet
- Anatomy 3.0: Anatomical EmbryologicalDocument49 pagesAnatomy 3.0: Anatomical EmbryologicalShenali SilvaNo ratings yet