You might also like
- Nursing care process in patients with chronic obstructive pulmonary diseaseFrom EverandNursing care process in patients with chronic obstructive pulmonary diseaseNo ratings yet
- Cold Sinus Sore Throat Tonsillitis Fever and Flu PDFDocument4 pagesCold Sinus Sore Throat Tonsillitis Fever and Flu PDFAnna GalánNo ratings yet
- Copd 2022Document45 pagesCopd 2022Mubassir NisarNo ratings yet
- Dyspnea - Chronic Obstructive Pulmonary DiseaseDocument64 pagesDyspnea - Chronic Obstructive Pulmonary Diseaseefe.uar59No ratings yet
- Vermilium JumpstartDocument14 pagesVermilium JumpstartFred FrançaNo ratings yet
- Gold and Gina Guideline For Copd and AsthmaDocument56 pagesGold and Gina Guideline For Copd and AsthmaSomnath Das GuptaNo ratings yet
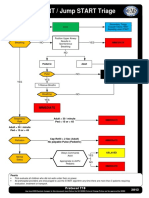
- Start - Jump START Triage PDFDocument2 pagesStart - Jump START Triage PDF081381246529100% (1)
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDocument49 pagesShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- Pain Management During LaborDocument30 pagesPain Management During LaborMary Ann Pardilla AlcoberNo ratings yet
- Dr. Reckeweg - R7Document2 pagesDr. Reckeweg - R7ManpreetSinghGrewalNo ratings yet
- EkgDocument121 pagesEkgElmir Tarani100% (1)
- Anesthesia Management in Bronchoscopy Procedure NewDocument29 pagesAnesthesia Management in Bronchoscopy Procedure NewChlara Obisuru100% (1)
- LiposuctionDocument14 pagesLiposuctionMaria BudnicNo ratings yet
- Introduction in Large Animal SurgeryDocument27 pagesIntroduction in Large Animal SurgeryDaisy LoussierNo ratings yet
- The Adult Client With Respiratory Disorder: 2017 EasalavanteDocument101 pagesThe Adult Client With Respiratory Disorder: 2017 EasalavanteNicholas TagleNo ratings yet
- Asthma and COPDDocument47 pagesAsthma and COPDSamuelVilbrunNo ratings yet
- Copd ReportDocument69 pagesCopd ReportRadley Jed C. PelagioNo ratings yet
- Acute Respiratory Failure For StudentDocument41 pagesAcute Respiratory Failure For Studentapi-379952350% (4)
- 13.acute Respiratory FailureDocument34 pages13.acute Respiratory Failurekarim hassan100% (1)
- Kum Peny Khusus COPD - DR - Indah SuhetyDocument20 pagesKum Peny Khusus COPD - DR - Indah SuhetyindahNo ratings yet
- Chronic Obstructive Airway Disease: Assoc Professor Dr. VinothiniDocument29 pagesChronic Obstructive Airway Disease: Assoc Professor Dr. VinothiniVivienneNo ratings yet
- Status AsmathicusDocument34 pagesStatus AsmathicuslarasNo ratings yet
- COPDDocument42 pagesCOPDAnoos rabayarabayaNo ratings yet
- Chronic Obstructive Pulmonary Disease: by Abhinay Sharma Bhugoo Ml-610Document62 pagesChronic Obstructive Pulmonary Disease: by Abhinay Sharma Bhugoo Ml-610abhinay_1712No ratings yet
- Respi CopdDocument90 pagesRespi CopdJosephine IsonNo ratings yet
- AsthmaDocument17 pagesAsthmashubhamz shaNo ratings yet
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Copd (Chronic Obstructive: Pulmonary Disease)Document68 pagesCopd (Chronic Obstructive: Pulmonary Disease)sinan kNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- Dr. Irbab HawariDocument25 pagesDr. Irbab HawariirbabhmdNo ratings yet
- Chronic Obstructive Pulmonary Disease: Joshi MarmikDocument27 pagesChronic Obstructive Pulmonary Disease: Joshi MarmikRaj DuraiNo ratings yet
- DR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedDocument47 pagesDR Josephine Ojoo Senior Lecturer Maseno University: MBCHB FRCP CCST (Resp) Dip Hiv MedMalueth AnguiNo ratings yet
- Approach To Chronic CoughDocument31 pagesApproach To Chronic CoughNoreen Ooi Zhi MinNo ratings yet
- Bronchodilators and Other Respiratory DrugsDocument44 pagesBronchodilators and Other Respiratory DrugsastriedamaliaamanatNo ratings yet
- ICU Management of COPD & Asthma 2Document35 pagesICU Management of COPD & Asthma 2Parvathy R Nair100% (1)
- Day 1 - APPEC 2021Document492 pagesDay 1 - APPEC 2021GaurieNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument45 pagesChronic Obstructive Pulmonary DiseaseAlexander Santiago ParelNo ratings yet
- Student Copy of COPD Lecture NotesDocument8 pagesStudent Copy of COPD Lecture NotesMary MarshNo ratings yet
- CopdDocument41 pagesCopdneelumshaukatNo ratings yet
- How To Manage VentilatorDocument31 pagesHow To Manage VentilatorValerie AnnekeNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Assistant Professor:Tong JinDocument39 pagesChronic Obstructive Pulmonary Disease (COPD) : Assistant Professor:Tong JinEINSTEIN2DNo ratings yet
- Acute Severe Asthma (Status Asthmaticus)Document20 pagesAcute Severe Asthma (Status Asthmaticus)blok etikakedokteranNo ratings yet
- Chronic Obstructive Pulmonary Disease: Olga Alexeevna EfremovaDocument56 pagesChronic Obstructive Pulmonary Disease: Olga Alexeevna Efremovaسيف الشمريNo ratings yet
- 1 - CopdDocument40 pages1 - Copdvmj8tyh5dsNo ratings yet
- CPAP SlidesDocument52 pagesCPAP SlidesAnusha Verghese100% (1)
- COPD CaseDocument73 pagesCOPD CaseTony DawaNo ratings yet
- Laparoscopy Morbid ThyroidDocument155 pagesLaparoscopy Morbid ThyroidparuNo ratings yet
- Post Intubation HypotensionDocument37 pagesPost Intubation Hypotensionfifa_0304535100% (1)
- COPDDocument49 pagesCOPDArmoured SpartanNo ratings yet
- Chest AyuDocument70 pagesChest AyuAbebe GelawNo ratings yet
- C.O.P.D: (Chronic Obstructive Pulmonary Disorder)Document47 pagesC.O.P.D: (Chronic Obstructive Pulmonary Disorder)KrystelNo ratings yet
- Clinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena AnjumDocument66 pagesClinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena Anjumgurrya786No ratings yet
- Copd ExacerbationDocument42 pagesCopd Exacerbationأبوأحمد الحكيمNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document23 pagesChronic Obstructive Pulmonary Disease (COPD)akoeljames8543No ratings yet
- Management of COPD ExacerbationDocument15 pagesManagement of COPD Exacerbationlitan dasNo ratings yet
- Chapter 4 HTDocument52 pagesChapter 4 HTtesfamichael mengistuNo ratings yet
- Chronic Obstructive Pulmonary Disease: Olivia Faye J Listanco IM Resident January 21, 2016Document52 pagesChronic Obstructive Pulmonary Disease: Olivia Faye J Listanco IM Resident January 21, 2016FayeListancoNo ratings yet
- Laparascopy PPOK DR YUDocument23 pagesLaparascopy PPOK DR YUAchmad MustikaNo ratings yet
- Acute Respiratory Distress SyndromeDocument24 pagesAcute Respiratory Distress SyndromePooja ShashidharanNo ratings yet
- Mechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDDocument25 pagesMechanical Ventilation: Weaning From Mechanical Ventilation Kathia Ortiz-Cantillo, MDsarevNo ratings yet
- Status Asthmaticus DR Divya JainDocument45 pagesStatus Asthmaticus DR Divya JainParvathy R NairNo ratings yet
- Dr. M Abdur Rahim M.D.,: Asst. Professor of MedicineDocument59 pagesDr. M Abdur Rahim M.D.,: Asst. Professor of Medicinemushtaq_23No ratings yet
- 3A 3B COPD With AnnotationsDocument42 pages3A 3B COPD With AnnotationsMangel Lucia MontecilloNo ratings yet
- Pulmonary EmphysemaDocument20 pagesPulmonary EmphysemaAbigailNo ratings yet
- 06 Respiratory03 Patho02Document46 pages06 Respiratory03 Patho02Divyajyoti DevaNo ratings yet
- Pemicu 6 KGD AditDocument76 pagesPemicu 6 KGD AditAditya SuksmawanNo ratings yet
- Case - Vii: AsthmaDocument18 pagesCase - Vii: AsthmaabubakarNo ratings yet
- 2-Shortness of Breath by DR - HananDocument49 pages2-Shortness of Breath by DR - HananSoon SheedNo ratings yet
- Analgesia & Sedation in ICU: OLEH: HidayatiDocument44 pagesAnalgesia & Sedation in ICU: OLEH: HidayatiZoelNo ratings yet
- ART Rugs and Nfusions: A. PolicyDocument7 pagesART Rugs and Nfusions: A. PolicyZoelNo ratings yet
- Daftar Pustaka KardiologiDocument4 pagesDaftar Pustaka KardiologiZoelNo ratings yet
- Orthopedic Surgery and Venous ThrombosisDocument7 pagesOrthopedic Surgery and Venous ThrombosisZoelNo ratings yet
- Orthopedic Surgery and Venous ThrombosisDocument30 pagesOrthopedic Surgery and Venous ThrombosisZoelNo ratings yet
- Anaesthetic Management of PheochromocytomaDocument22 pagesAnaesthetic Management of PheochromocytomaZoelNo ratings yet
- Cosmetic Surgery: Concerns About Anesthesia: 362 Fairlawn Avenue Toronto, ON M5M 1T6 (647) 931-5358Document3 pagesCosmetic Surgery: Concerns About Anesthesia: 362 Fairlawn Avenue Toronto, ON M5M 1T6 (647) 931-5358ZoelNo ratings yet
- DPJP: Dr. Fachrul Jamal, SP - An-Kic.: 3 Rencana AnestesiDocument7 pagesDPJP: Dr. Fachrul Jamal, SP - An-Kic.: 3 Rencana AnestesiZoelNo ratings yet
- 1 s2.0 S1743919115003684 MainDocument6 pages1 s2.0 S1743919115003684 MainZoelNo ratings yet
- DPJP: Dr. T. Yasir, SP - An-KIC. 3 Rencana AnestesiDocument7 pagesDPJP: Dr. T. Yasir, SP - An-KIC. 3 Rencana AnestesiZoelNo ratings yet
- Anesthesia For Orthopedic, Ent and Maxillofacial Surgery: Presented by-DR - POOJA Moderator-DR - GIRISH SHARMADocument47 pagesAnesthesia For Orthopedic, Ent and Maxillofacial Surgery: Presented by-DR - POOJA Moderator-DR - GIRISH SHARMAZoelNo ratings yet
- List BUKU TEXT (TEXT BOOK) Di Ruang BacaDocument3 pagesList BUKU TEXT (TEXT BOOK) Di Ruang BacaZoelNo ratings yet
- Anesthesia For Laparoscopic Surgeries: Prepared & Presented By: Dr. Roshana MallawaarachchiDocument53 pagesAnesthesia For Laparoscopic Surgeries: Prepared & Presented By: Dr. Roshana MallawaarachchiZoelNo ratings yet
- Turp Syndrome: Dr. Mahyal Habibi 1607601080001Document10 pagesTurp Syndrome: Dr. Mahyal Habibi 1607601080001ZoelNo ratings yet
- PRCL Research PaperDocument4 pagesPRCL Research PaperDevisha MehrotraNo ratings yet
- Biology ThesisDocument25 pagesBiology ThesisValli RamalingamNo ratings yet
- Schistosoma Lecture OutlineDocument2 pagesSchistosoma Lecture OutlineMershen GaniaNo ratings yet
- Materi - Confounders in Internal Validity - GM IPBDocument21 pagesMateri - Confounders in Internal Validity - GM IPBsalehahnhNo ratings yet
- Guidelines For The Management of Congenital Heart Diseases in CH 2017Document105 pagesGuidelines For The Management of Congenital Heart Diseases in CH 2017Ludwig CaceresNo ratings yet
- Instant Download Course in Probability 1st Edition Weiss Solutions Manual PDF Full ChapterDocument33 pagesInstant Download Course in Probability 1st Edition Weiss Solutions Manual PDF Full Chapterwilliammaximilian16jvl100% (8)
- 6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma TasksDocument20 pages6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma TasksMiguel CosteNo ratings yet
- Amtrak Vaccine MandateDocument2 pagesAmtrak Vaccine MandateAnna SaundersNo ratings yet
- BPL Catlogue Updated With 3dDocument24 pagesBPL Catlogue Updated With 3dcpt abbasNo ratings yet
- 201217Document7 pages201217dr anilaNo ratings yet
- Cell Division Is The Basis of Reproduction For Every OrganismDocument3 pagesCell Division Is The Basis of Reproduction For Every OrganismAlliah MendozaNo ratings yet
- McGill Nutrition Guide Page8 Homemade Food SupplementsDocument31 pagesMcGill Nutrition Guide Page8 Homemade Food Supplementsapi-3714923100% (1)
- Catalog-2021 - en - A4Document22 pagesCatalog-2021 - en - A4vw5ohgjrNo ratings yet
- Acute AbdomenDocument125 pagesAcute Abdomenvinitha kattaNo ratings yet
- Joshi Abhishek Ashvinbhai S.Y.P.B.B.Sc - Nursing Gov - College of Nursing JamnagarDocument123 pagesJoshi Abhishek Ashvinbhai S.Y.P.B.B.Sc - Nursing Gov - College of Nursing JamnagarKristine C.No ratings yet
- Chronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewDocument5 pagesChronic Kidney Disease (CKD) - McMaster Pathophysiology ReviewAnonymous uziTjed5j100% (1)
- Symptom Management: Chapter Four Denim E. MaghanoyDocument32 pagesSymptom Management: Chapter Four Denim E. MaghanoyDenim Embalzado MaghanoyNo ratings yet
- The Neuronal EnvironmentDocument428 pagesThe Neuronal EnvironmentPandaNo ratings yet
- Bed Bug Fumigation Check List3Document3 pagesBed Bug Fumigation Check List3desibanda73No ratings yet
- Animal ModelsDocument22 pagesAnimal ModelsM.anwar KhanNo ratings yet
- Pune CME 2011 BrochureDocument4 pagesPune CME 2011 BrochuredrpajaniNo ratings yet
- Lesson Plan On Theory.Document12 pagesLesson Plan On Theory.Bhumi ChouhanNo ratings yet