You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- NSEM MergedDocument142 pagesNSEM Mergedczeremar chanNo ratings yet
- Group 1 BSN 3a Final Compiled RequirementsDocument37 pagesGroup 1 BSN 3a Final Compiled Requirementsczeremar chanNo ratings yet
- Emergency Pediatric CareDocument1 pageEmergency Pediatric Careczeremar chanNo ratings yet
- BLS Skills Lab For SimulationDocument116 pagesBLS Skills Lab For Simulationczeremar chan100% (1)
- Chole CystitisDocument13 pagesChole CystitisColdicedNo ratings yet
- The Application of A Continuous Strip of Woven Material To A Body PartDocument15 pagesThe Application of A Continuous Strip of Woven Material To A Body Partczeremar chanNo ratings yet
- Med Case StudyDocument113 pagesMed Case Studyczeremar chanNo ratings yet
- Group 1 BSN3A Final IMRAD PaperDocument134 pagesGroup 1 BSN3A Final IMRAD Paperczeremar chanNo ratings yet
- Management-Notes ncm119Document2 pagesManagement-Notes ncm119czeremar chanNo ratings yet
- LEADERSHIP AND MANAGEMENT Notes 1Document3 pagesLEADERSHIP AND MANAGEMENT Notes 1czeremar chanNo ratings yet
- TRIAGE Skills LabDocument8 pagesTRIAGE Skills Labczeremar chanNo ratings yet
- Medical or Pedia or Surgical Case Study Format GROUP 1Document3 pagesMedical or Pedia or Surgical Case Study Format GROUP 1czeremar chanNo ratings yet
- Digest This!Document7 pagesDigest This!Dhen MarcNo ratings yet
- Kdigo 2012 CKD GLDocument163 pagesKdigo 2012 CKD GLOkky Sari Rahayu100% (1)
- NCM 119 PrelimDocument12 pagesNCM 119 Prelimczeremar chan100% (1)
- Macrolide Antibiotics: BeforeDocument3 pagesMacrolide Antibiotics: Beforeczeremar chanNo ratings yet
- Republic Act 9173 Philippine Nursing Act of 2002: Why We Have RA 9173?Document7 pagesRepublic Act 9173 Philippine Nursing Act of 2002: Why We Have RA 9173?czeremar chan100% (1)
- ADVOCACY: "Healthier Nurses, Healthier Patients" Objective:: Christine Elbanbuena Czeremar Chan Bsn4ADocument1 pageADVOCACY: "Healthier Nurses, Healthier Patients" Objective:: Christine Elbanbuena Czeremar Chan Bsn4Aczeremar chanNo ratings yet
- Are Quiet Alarms, Real-Time Advice and AI The Future of Intensive Care?Document6 pagesAre Quiet Alarms, Real-Time Advice and AI The Future of Intensive Care?czeremar chanNo ratings yet
- Cefuroxime Drug Study ChanDocument5 pagesCefuroxime Drug Study Chanczeremar chanNo ratings yet
- Assiting Patient To Use Assistive Devices For Walking PDFDocument10 pagesAssiting Patient To Use Assistive Devices For Walking PDFczeremar chanNo ratings yet
- Antineoplastic AgentsDocument13 pagesAntineoplastic Agentsczeremar chanNo ratings yet
- Antineoplastic AgentsDocument13 pagesAntineoplastic Agentsczeremar chanNo ratings yet
- Drug StudyDocument3 pagesDrug Studyczeremar chanNo ratings yet
- Drug StudyDocument3 pagesDrug Studyczeremar chanNo ratings yet
- Drug StudyDocument3 pagesDrug Studyczeremar chanNo ratings yet
- Concept Paper Research TitleDocument10 pagesConcept Paper Research Titleczeremar chanNo ratings yet
- NCM 111 Research 1 Midterm by Xerxes G. Malaga, RN, MNDocument14 pagesNCM 111 Research 1 Midterm by Xerxes G. Malaga, RN, MNczeremar chanNo ratings yet
- Nurse in The National and Global Health Care Delivery SystemDocument9 pagesNurse in The National and Global Health Care Delivery Systemczeremar chanNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Antibiotic Susceptibility of Bacterial Isolates FRDocument8 pagesAntibiotic Susceptibility of Bacterial Isolates FRkaren leeNo ratings yet
- Reducing Infant MortalityDocument2 pagesReducing Infant MortalitySara FrazierNo ratings yet
- Douglas K. Blacklidge, DPM Home Address: 3072 West 250 SouthDocument6 pagesDouglas K. Blacklidge, DPM Home Address: 3072 West 250 SouthbaoNo ratings yet
- Toacs Surgical Trainees 2009 ADocument15 pagesToacs Surgical Trainees 2009 AAnonymous bzHRfZzv100% (1)
- Autoimmune Diseases: Dr. Ansar Uddin Ahmed Asst. Prof and Head Dept. of Periodontology and Oral PathologyDocument13 pagesAutoimmune Diseases: Dr. Ansar Uddin Ahmed Asst. Prof and Head Dept. of Periodontology and Oral PathologyTas DidNo ratings yet
- ESL Brains What Should We Be Afraid of SVDocument3 pagesESL Brains What Should We Be Afraid of SVMafe NomásNo ratings yet
- Self Assessment / Checklist FormDocument1 pageSelf Assessment / Checklist FormAiza Rhea SantosNo ratings yet
- International Journal of Pharmaceutics: Yuqing Ye, Ying Ma, Jesse ZhuDocument17 pagesInternational Journal of Pharmaceutics: Yuqing Ye, Ying Ma, Jesse ZhuAlina CiugureanuNo ratings yet
- TFN Dorothea OremDocument22 pagesTFN Dorothea OremRaphael SevillaNo ratings yet
- EDIC Guidelines 2009 Version October 09Document7 pagesEDIC Guidelines 2009 Version October 09Mubarak Elradi NourNo ratings yet
- Paper: Volodymyr A. Vinnikov and Oleg BelyakovDocument12 pagesPaper: Volodymyr A. Vinnikov and Oleg BelyakovMalik AzeemNo ratings yet
- Core Stability JournalDocument12 pagesCore Stability JournalfricaNo ratings yet
- Responsibilities of A CRADocument15 pagesResponsibilities of A CRAapi-3810976No ratings yet
- USFDA A To Z DefinationDocument26 pagesUSFDA A To Z DefinationRishikesh ChakorNo ratings yet
- RSSDI - Practice GuideDocument29 pagesRSSDI - Practice Guidechinnu prakash100% (1)
- Polemics and Pregnancy: A Response To Arguments About Ethical Obstetrical CareDocument3 pagesPolemics and Pregnancy: A Response To Arguments About Ethical Obstetrical CareMuhammad Ikhwanul HakimNo ratings yet
- Expiratory Cassette Cleaning Wall Manual PDFDocument4 pagesExpiratory Cassette Cleaning Wall Manual PDFmatzone0% (3)
- Blue and Yellow Minimalist Employee of The Month Certificate PDFDocument20 pagesBlue and Yellow Minimalist Employee of The Month Certificate PDFKizzy Ann PenaverdeNo ratings yet
- Medical Billing Questions 1Document7 pagesMedical Billing Questions 1framar572112100% (1)
- Leaflet Terhadap Kecemasan Keluarga Pasien LabelDocument12 pagesLeaflet Terhadap Kecemasan Keluarga Pasien LabelYehezkiel DwiNo ratings yet
- World Health Champion Game Questions and Answers BRMDocument18 pagesWorld Health Champion Game Questions and Answers BRMNourhan YehiaNo ratings yet
- Clinical Guidelines On IYCF - 1Document37 pagesClinical Guidelines On IYCF - 1ইসরাত বারীNo ratings yet
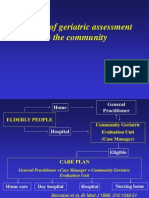
- The Use of Geriatric Assessment in The CommunityDocument16 pagesThe Use of Geriatric Assessment in The Communityhendra2darmawanNo ratings yet
- Michelle Martin Resume 2021 Final 1pageDocument1 pageMichelle Martin Resume 2021 Final 1pageapi-540444992No ratings yet
- GliffozinasDocument11 pagesGliffozinasArahiMaflaNo ratings yet
- “They just don’t like to wait”--A comparative study of Aboriginal and non-Aboriginal people who did not wait for treatment or discharged against medical advice from rural emergency departments- Part 1.PDFDocument8 pages“They just don’t like to wait”--A comparative study of Aboriginal and non-Aboriginal people who did not wait for treatment or discharged against medical advice from rural emergency departments- Part 1.PDFLikhna PertiwiNo ratings yet
- ICD 10 Dalam ExcelDocument103 pagesICD 10 Dalam ExcelJumpa Utama AmrannurNo ratings yet
- ReproTech, LLC Welcomes New President & CEO, William BraunDocument3 pagesReproTech, LLC Welcomes New President & CEO, William BraunPR.comNo ratings yet
- Production of NDV Using Propagation of Vero Cells For Vaccine DevelopmentDocument1 pageProduction of NDV Using Propagation of Vero Cells For Vaccine DevelopmentRiduan NightrayNo ratings yet
- Classical Five-Element Acupuncture: Two More Powerful Treatment StrategiesDocument10 pagesClassical Five-Element Acupuncture: Two More Powerful Treatment StrategiesANo ratings yet