You might also like
- Dr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaDocument30 pagesDr. Padma Bhatia: Assistant Professor Department of Community Medicine G.M.C., Bhopal. M.P. IndiaSakshi SuriNo ratings yet
- BHIM 024 Healthcare Financing PDFDocument28 pagesBHIM 024 Healthcare Financing PDFpalak maheshwariNo ratings yet
- Health EconomicsDocument19 pagesHealth EconomicsSwati SharmaNo ratings yet
- Group B Presentation 2Document40 pagesGroup B Presentation 2Doaa AwadNo ratings yet
- 2023 MBCHB Health Financing and Provider Payment MechanismsDocument59 pages2023 MBCHB Health Financing and Provider Payment MechanismsKELLY KIPKOECHNo ratings yet
- Health Care Financing: Preethi PradhanDocument21 pagesHealth Care Financing: Preethi PradhanRoHIT ShowNo ratings yet
- Group Presentation on Various Aspects of InsuranceDocument14 pagesGroup Presentation on Various Aspects of InsuranceHimanshuNo ratings yet
- Report On Health Insurance 2Document23 pagesReport On Health Insurance 2DrJaideep KumarNo ratings yet
- Session 7 Health Care Finanancing (Compatibility Mode)Document36 pagesSession 7 Health Care Finanancing (Compatibility Mode)Behar AbdurahemanNo ratings yet
- Unit 4Document63 pagesUnit 4Narrainshree SathiyarajeswaranNo ratings yet
- Neha BKDocument46 pagesNeha BKpiyushborade143No ratings yet
- BSC II Health Financing in UgandaDocument25 pagesBSC II Health Financing in UgandaYusto FoshizoNo ratings yet
- Health Insurance in India-An Overview: K.Swathi, R.AnuradhaDocument4 pagesHealth Insurance in India-An Overview: K.Swathi, R.AnuradhaAnkit YadavNo ratings yet
- HEALTH INSURANCE OPTIONS IN INDIADocument10 pagesHEALTH INSURANCE OPTIONS IN INDIADevendra SawantNo ratings yet
- Health InsuranceDocument28 pagesHealth InsuranceMajibul Rehman86% (7)
- Chapter 1: Introduction of The Project: Health InsuranceDocument62 pagesChapter 1: Introduction of The Project: Health Insuranceapeksha bhoirNo ratings yet
- Health Care Financing: Characteristics / Approaches and MethodsDocument18 pagesHealth Care Financing: Characteristics / Approaches and MethodsSOOMA OSMANNo ratings yet
- International Social Welfare ProgramsDocument10 pagesInternational Social Welfare ProgramsZaira Edna JoseNo ratings yet
- Emerging Health Insurance in India-An Overview - J AnithaDocument17 pagesEmerging Health Insurance in India-An Overview - J AnithaSwayam Suraj NayakNo ratings yet
- Health Insurance: Pramod KumarDocument21 pagesHealth Insurance: Pramod KumarSuneel Kumar PrajapatiNo ratings yet
- COMMED - Healthcare Financing 2008Document60 pagesCOMMED - Healthcare Financing 2008api-3856051100% (1)
- 5.basic Principles of Health Economics - Health Care FinancingDocument21 pages5.basic Principles of Health Economics - Health Care FinancingBENDOR MOSESNo ratings yet
- Mckinsey 2007 Global Persspectives On Indian Health InsDocument72 pagesMckinsey 2007 Global Persspectives On Indian Health InsharihfamNo ratings yet
- Health SystemDocument7 pagesHealth SystemkatieminnixNo ratings yet
- Health Financing Reform in Uganda: How Equitable Is The Proposed National Health Insurance Scheme?Document8 pagesHealth Financing Reform in Uganda: How Equitable Is The Proposed National Health Insurance Scheme?Byaruhanga EmmanuelNo ratings yet
- Health InsurancesDocument7 pagesHealth InsurancesGlorina KumarNo ratings yet
- Health Insurance LawDocument16 pagesHealth Insurance LawParul NayakNo ratings yet
- Financing Health ServicesDocument16 pagesFinancing Health ServicesMahdi SwaidanNo ratings yet
- 2nd Shreet Report of KavyaDocument70 pages2nd Shreet Report of KavyaKavya NaikNo ratings yet
- IRDA IC 38 (17 21) Refresher 2Document12 pagesIRDA IC 38 (17 21) Refresher 2Anant PandeyNo ratings yet
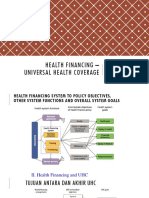
- Pembiayaan Kesehatan UHCDocument43 pagesPembiayaan Kesehatan UHCGenre PesselNo ratings yet
- Current Scenario of Health Insurance in India: A Study Comprising Various Challenges and Measures For ITDocument7 pagesCurrent Scenario of Health Insurance in India: A Study Comprising Various Challenges and Measures For ITEditor IJTSRDNo ratings yet
- Healthcare Insurance Evolution in India An Opportunity To Expand AccessDocument7 pagesHealthcare Insurance Evolution in India An Opportunity To Expand AccessCherylAlishaD'SouzaNo ratings yet
- Creating Consumer Awareness in Life InsuranceDocument63 pagesCreating Consumer Awareness in Life Insurancepinki2211No ratings yet
- Health Insurance Sector in IndiaDocument11 pagesHealth Insurance Sector in IndiaPanimalar Engineering College MBANo ratings yet
- Health Insurance Nsg Mgt Seminar-IIDocument43 pagesHealth Insurance Nsg Mgt Seminar-IIdivya rajasekaranNo ratings yet
- Functions of Health FinancingDocument35 pagesFunctions of Health FinancingShrestha SharmilaNo ratings yet
- Health Law ProjectDocument22 pagesHealth Law ProjectVarun MittalNo ratings yet
- Submitted To: - Submitted By:-Ms. Taru Baswan Asha (Lecturer) Prateek Agarwal Shanky GuptaDocument18 pagesSubmitted To: - Submitted By:-Ms. Taru Baswan Asha (Lecturer) Prateek Agarwal Shanky GuptaShanky GuptaNo ratings yet
- Australia - International Health Care System ProfilesDocument10 pagesAustralia - International Health Care System ProfilesAboubacar SompareNo ratings yet
- Health Financing MethodsDocument3 pagesHealth Financing MethodsMuna Hassan MustafaNo ratings yet
- I Am Sharing 'Introdu 13' With YouDocument38 pagesI Am Sharing 'Introdu 13' With Youbincybabuu87No ratings yet
- Health Insurance in IndiaDocument93 pagesHealth Insurance in IndiaSaurabh NagwekarNo ratings yet
- Health Insurance Case Study - RAS Scheme AnalysisDocument4 pagesHealth Insurance Case Study - RAS Scheme AnalysisRitesh KumarNo ratings yet
- Healthcar space managementDocument24 pagesHealthcar space managementseife slassieNo ratings yet
- Third Party AdministratorsDocument8 pagesThird Party Administratorsmanoj_pareek_3No ratings yet
- Herbert - Nyirenda 1590992698 ADocument39 pagesHerbert - Nyirenda 1590992698 ADavid LyeluNo ratings yet
- Social Health Insurance in India Current ScenarioDocument22 pagesSocial Health Insurance in India Current ScenarioRohit MalviyaNo ratings yet
- Thinking of Introducing Social Health Insurance? Ten QuestionsDocument10 pagesThinking of Introducing Social Health Insurance? Ten QuestionsIraaNo ratings yet
- Community-Based Health InsuranceDocument35 pagesCommunity-Based Health Insuranceyakubu I saidNo ratings yet
- Knight Riders - IIM Kozhikode - Optum PrimeDocument14 pagesKnight Riders - IIM Kozhikode - Optum PrimeASHWINI KUMAR 22No ratings yet
- Project Report On Health Law: Limitations On Liabilities and MediclaimDocument17 pagesProject Report On Health Law: Limitations On Liabilities and MediclaimDeepesh SinghNo ratings yet
- 2.1. Definition of Health Care SystemDocument12 pages2.1. Definition of Health Care SystemSittie Aina MunderNo ratings yet
- Personal and Business Risk MGMTDocument50 pagesPersonal and Business Risk MGMTYuba Raj DahalNo ratings yet
- FinalDocument61 pagesFinalAJAYYOGESHSHARMA100% (1)
- Health Care in Canada Has Long Been A Source of National PrideDocument24 pagesHealth Care in Canada Has Long Been A Source of National PridecadecortxNo ratings yet
- Health InsuranceDocument24 pagesHealth InsuranceMd Emroz Hossain100% (1)
- Safeshop BrochureDocument17 pagesSafeshop BrochurePrasanjeet BhattacharjeeNo ratings yet
- Direct SellingDocument94 pagesDirect SellingRadhika AroraNo ratings yet
- Thematic Note On Indian Hair Oil CategorDocument42 pagesThematic Note On Indian Hair Oil CategorPrasanjeet BhattacharjeeNo ratings yet
- Is your insurance complaint unheard? Contact IRDA for helpDocument10 pagesIs your insurance complaint unheard? Contact IRDA for helpvinaysekharNo ratings yet
- Aster Soaps HighlightsDocument1 pageAster Soaps HighlightsPrasanjeet BhattacharjeeNo ratings yet
- List of Tehsils in IndiaDocument11 pagesList of Tehsils in IndiaPrasanjeet Bhattacharjee100% (1)
- Product Catalogue India English PDFDocument100 pagesProduct Catalogue India English PDFDashrath menariyaNo ratings yet
- Salient Features of The Revised Irr OF R.A. 9520Document21 pagesSalient Features of The Revised Irr OF R.A. 9520AJ NaragNo ratings yet
- Data Privacy Consent FormDocument1 pageData Privacy Consent FormAraceli Gloria100% (2)
- Adamjee Internship Report by Aftab AliDocument11 pagesAdamjee Internship Report by Aftab AliAftab AliNo ratings yet
- INSURANCE - Sun Life Assurance - Vs - CA and Sps. BacaniDocument2 pagesINSURANCE - Sun Life Assurance - Vs - CA and Sps. Bacanimichelle zatarainNo ratings yet
- Solution Manual For Business Law Today Comprehensive 12th Edition Roger Leroy MillerDocument13 pagesSolution Manual For Business Law Today Comprehensive 12th Edition Roger Leroy MillerCameronHerrerayfep100% (39)
- Marine QuoteDocument9 pagesMarine QuotehiteshNo ratings yet
- 15 Malayan Insurance v. LinDocument2 pages15 Malayan Insurance v. LinRoger Montero Jr.No ratings yet
- Financial Risk Management Instruments for Renewable Energy Projects in Developing CountriesDocument118 pagesFinancial Risk Management Instruments for Renewable Energy Projects in Developing CountriessyoussefNo ratings yet
- State of New Jersey Department of Labor and Workforce DevelopmentDocument52 pagesState of New Jersey Department of Labor and Workforce DevelopmentMaria ENo ratings yet
- Residential Rental Property GuideDocument31 pagesResidential Rental Property GuideArnold GalvanNo ratings yet
- The Fintech 250Document65 pagesThe Fintech 250loticamoNo ratings yet
- Trends and developments in the Indian general insurance sectorDocument26 pagesTrends and developments in the Indian general insurance sectorrajNo ratings yet
- Bajaj Bike 2021Document2 pagesBajaj Bike 2021sarath potnuriNo ratings yet
- Medical Expenses Claim FormDocument4 pagesMedical Expenses Claim FormCHEMA KREMANo ratings yet
- Praxis 2011Document72 pagesPraxis 2011zhuhainie0% (1)
- Getting Started: Public Finance Manual SolutionsDocument92 pagesGetting Started: Public Finance Manual SolutionsChan ZacharyNo ratings yet
- Income from House Property CalculationDocument14 pagesIncome from House Property CalculationSarvar Pathan100% (3)
- Smart Wealth Assure - BrochureDocument16 pagesSmart Wealth Assure - BrochureIswarya SelvarajNo ratings yet
- Comparison Study Between Sunfeast and Britannia Biscuits: Scope of The StudyDocument36 pagesComparison Study Between Sunfeast and Britannia Biscuits: Scope of The StudygoudarameshvNo ratings yet
- GCC Healthcare Sector Poised for Strong GrowthDocument59 pagesGCC Healthcare Sector Poised for Strong GrowthToni Rose RotulaNo ratings yet
- Brochure Young Star Insurance PolicyDocument15 pagesBrochure Young Star Insurance PolicyAbhishek ANo ratings yet
- Case Study Asc302Document17 pagesCase Study Asc302Izzah Batrisyia Khairul HadiNo ratings yet
- Prime Life Insurance LimitedDocument36 pagesPrime Life Insurance LimitedFaquir Sanoar SanyNo ratings yet
- Incubator Business Plan: City of Auburn, WaDocument22 pagesIncubator Business Plan: City of Auburn, WaSudeep BeheraNo ratings yet
- Phil. Home Assurance Corp vs. CADocument1 pagePhil. Home Assurance Corp vs. CACaroline A. LegaspinoNo ratings yet
- What Is Corporate Banking PDFDocument2 pagesWhat Is Corporate Banking PDFSonakshi Behl100% (1)
- Insurance policy dispute over property transfer locationDocument6 pagesInsurance policy dispute over property transfer locationDis CatNo ratings yet
- Terrain Park DesignsDocument9 pagesTerrain Park Designsapi-285183593No ratings yet
- Finman General Assurance CorporationDocument2 pagesFinman General Assurance CorporationSernande PenNo ratings yet
- Whole life insurance explainedDocument15 pagesWhole life insurance explainedEmir AdemovicNo ratings yet