You might also like
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordFrom EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordNo ratings yet
- Running Head: PROJECT ASSIGNMENT 4 1Document13 pagesRunning Head: PROJECT ASSIGNMENT 4 1Farasha SSNo ratings yet
- Newman's Certified Electronic Health Records Technician Study GuideFrom EverandNewman's Certified Electronic Health Records Technician Study GuideNo ratings yet
- Journal of Biomedical InformaticsDocument11 pagesJournal of Biomedical InformaticsLuna Fitria KusumaNo ratings yet
- Cognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareFrom EverandCognitive Informatics: Reengineering Clinical Workflow for Safer and More Efficient CareKai ZhengNo ratings yet
- Xiao DevelopmentToolMeasure 2014Document7 pagesXiao DevelopmentToolMeasure 2014sysokuvaNo ratings yet
- Final PDFDocument18 pagesFinal PDFapi-655449085No ratings yet
- Running Head: Cost-Benefit Analysis of Electronic Health RecordsDocument11 pagesRunning Head: Cost-Benefit Analysis of Electronic Health RecordsBilal Ahmad BhatNo ratings yet
- Using The Decomposed Theory of Planned Behaviour To Explain Healthcare Consumer Adoption of Electronic Health RecordsDocument10 pagesUsing The Decomposed Theory of Planned Behaviour To Explain Healthcare Consumer Adoption of Electronic Health RecordsBekele Guta GemeneNo ratings yet
- Ehr Poster 1 1Document1 pageEhr Poster 1 1api-542441070No ratings yet
- Project 2Document13 pagesProject 2Abdulrahaman AbdulraheemNo ratings yet
- Newsletter and RP STARTDocument4 pagesNewsletter and RP STARTBálint ÁrpádNo ratings yet
- Optimizing The Electronic Health Records Through BDocument10 pagesOptimizing The Electronic Health Records Through BZara AkbariNo ratings yet
- Order ### 2672790Document11 pagesOrder ### 2672790Wallace Mandela Ong'ayoNo ratings yet
- CHAPTER TWO LITERATURE REVIEW (Roles of EMR Project)Document5 pagesCHAPTER TWO LITERATURE REVIEW (Roles of EMR Project)bonfaceNo ratings yet
- (Gagnon Et Al., 2003) An Adaptation of The Theory of Interpersonal Behaviour To The Study of Telemedicine Adoption by PhysiciansDocument13 pages(Gagnon Et Al., 2003) An Adaptation of The Theory of Interpersonal Behaviour To The Study of Telemedicine Adoption by Physiciansrhizom cruzNo ratings yet
- Nursing Informatics Week-12-13Document37 pagesNursing Informatics Week-12-13astraeax pandaNo ratings yet
- CH 11 - Ehr ActivityDocument4 pagesCH 11 - Ehr ActivityJAY LORENZ CARIDONo ratings yet
- Hlthaff 2010 0557 PDFDocument10 pagesHlthaff 2010 0557 PDFAnonymousNo ratings yet
- Abstract VFDocument2 pagesAbstract VFElite TutorNo ratings yet
- NUR502 Discussion5Document3 pagesNUR502 Discussion5audleyNo ratings yet
- Hcin 540 EssayDocument14 pagesHcin 540 Essayapi-408487557No ratings yet
- Running Head: Health Information Technology 1Document12 pagesRunning Head: Health Information Technology 1api-469824583No ratings yet
- Electronic Health Record Implementation StrategiesDocument10 pagesElectronic Health Record Implementation StrategiesATS100% (1)
- Physicians and Nurses Experiences On EHR Usability - 2020 - International JouDocument9 pagesPhysicians and Nurses Experiences On EHR Usability - 2020 - International JouRobotNo ratings yet
- f3d3 PDFDocument40 pagesf3d3 PDFSiti QamariaNo ratings yet
- Matic Pablo Pantig Patungan Peralta Nursing Informatics Final Requirement Conduct of Research Writing Thru Scoping ReviewDocument11 pagesMatic Pablo Pantig Patungan Peralta Nursing Informatics Final Requirement Conduct of Research Writing Thru Scoping ReviewYuuki Chitose (tai-kun)No ratings yet
- Chapter 14Document23 pagesChapter 14Kristia Noelle FranciscoNo ratings yet
- The Integration and Appraisal of Electronic Medical Records (EMR)Document4 pagesThe Integration and Appraisal of Electronic Medical Records (EMR)Leah FlorentinoNo ratings yet
- CCN Final SubmissionDocument8 pagesCCN Final SubmissionnishuNo ratings yet
- Benefits and Drawbacks of Electronic Health Record SystemsDocument10 pagesBenefits and Drawbacks of Electronic Health Record Systemstylermichael912No ratings yet
- CernerDocument10 pagesCernerazul2233No ratings yet
- Research ArticleDocument25 pagesResearch ArticleDanoe SoesantoNo ratings yet
- PredictiveDocument11 pagesPredictivesansNo ratings yet
- Tugas Share 3Document23 pagesTugas Share 3FitriNo ratings yet
- Proposal 023629-1Document12 pagesProposal 023629-1ADEOYE JAMESNo ratings yet
- The Impact of Computerized Provider Order Entry On Nursing PracticeDocument6 pagesThe Impact of Computerized Provider Order Entry On Nursing PracticeWella Pasya DheaNo ratings yet
- Health Care Provider Adoption of EHealthDocument22 pagesHealth Care Provider Adoption of EHealthvoNo ratings yet
- Electronic Health Record Management ExpeDocument5 pagesElectronic Health Record Management Expetylermichael912No ratings yet
- Electronic Medical Record/Electronic Health Record System: Problem Based LearningDocument13 pagesElectronic Medical Record/Electronic Health Record System: Problem Based LearningTonmoy Banerjee100% (1)
- The Adoption of Technology Orientation in Healthcare DeliveryDocument20 pagesThe Adoption of Technology Orientation in Healthcare DeliveryAsparagusJr JuniorNo ratings yet
- JMDH 14 2597Document7 pagesJMDH 14 2597PutriiNo ratings yet
- EHR PerceptionsDocument27 pagesEHR Perceptionspearl ikebuakuNo ratings yet
- STRATEGY FOR SUCCESSFUL ACCELERATION OF USAGE - Submit3Document7 pagesSTRATEGY FOR SUCCESSFUL ACCELERATION OF USAGE - Submit3IdaNo ratings yet
- Review Paper PDFDocument9 pagesReview Paper PDFbhushaninjeNo ratings yet
- Hcin 540 - Finished Final Project PDFDocument12 pagesHcin 540 - Finished Final Project PDFapi-562816202No ratings yet
- Ratwani Electronic Health Records and Improved Patient CareDocument11 pagesRatwani Electronic Health Records and Improved Patient CareSibli AhmadNo ratings yet
- Nancy Kamau PDFDocument47 pagesNancy Kamau PDFAri Azhari100% (1)
- EHR Adoption and Hospital Performance: Time-Related Effects: Julia Adler-Milstein, Jordan Everson, and Shoou-Yih D. LeeDocument21 pagesEHR Adoption and Hospital Performance: Time-Related Effects: Julia Adler-Milstein, Jordan Everson, and Shoou-Yih D. LeesinggihwpNo ratings yet
- Social Capital and Transaction Cost On Co-Creating IT Value Towardsinter-Organizational EMR ExchangeDocument14 pagesSocial Capital and Transaction Cost On Co-Creating IT Value Towardsinter-Organizational EMR ExchangeKiyoshi Naito VegaNo ratings yet
- Kemloh, 330Document10 pagesKemloh, 330mohamedNo ratings yet
- Benefits - and - Challenges - of - Ele 6Document7 pagesBenefits - and - Challenges - of - Ele 6silfianaNo ratings yet
- Ehr ThesisDocument8 pagesEhr Thesisjenniferlopezhayward100% (1)
- Informatics RaveloDocument4 pagesInformatics RaveloKyle Isidro MaleNo ratings yet
- Improving Quality Through Effective Implementation of Information Technology in HealthcareDocument8 pagesImproving Quality Through Effective Implementation of Information Technology in HealthcareSai VishnuNo ratings yet
- EHR Adv and DisadvantagesDocument7 pagesEHR Adv and DisadvantagesIvibe mashNo ratings yet
- HealthcareDocument8 pagesHealthcareAnas BilalNo ratings yet
- E Sağlık Kullanımında Hasta Hekim IlişkisiDocument6 pagesE Sağlık Kullanımında Hasta Hekim IlişkisimumtazkorkutanNo ratings yet
- NX Info Reporting Dump PDFDocument11 pagesNX Info Reporting Dump PDFJar JeonNo ratings yet
- Medicatikon ErrorDocument13 pagesMedicatikon ErrorArdi NugrohoNo ratings yet
- LCP Reflection PaperDocument3 pagesLCP Reflection PaperGhea GatingaNo ratings yet
- Lrfdseis 2 I3Document9 pagesLrfdseis 2 I3KY PengNo ratings yet
- Harrison - Naturalism and Success of ScienceDocument18 pagesHarrison - Naturalism and Success of ScienceDi WuNo ratings yet
- Dwnload Full Television Production Handbook 11th Edition Zettl Test Bank PDFDocument35 pagesDwnload Full Television Production Handbook 11th Edition Zettl Test Bank PDFanimismmildpkajkl100% (8)
- Vbscript ExemplosDocument6 pagesVbscript ExemplosRogelio E. SabrinaNo ratings yet
- Sample ProblemsDocument3 pagesSample ProblemsSwati SatyendraNo ratings yet
- 51320062004AL-FFU130HAX (L - MBP) - DatasheetDocument4 pages51320062004AL-FFU130HAX (L - MBP) - Datasheetdesenvolvimento appNo ratings yet
- Lok 2015Document214 pagesLok 2015JasmineTYPNo ratings yet
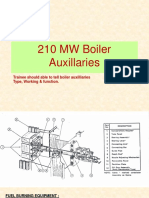
- 210 MW Boiler AuxillariesDocument18 pages210 MW Boiler AuxillariesAhemadNo ratings yet
- ECE 442 Electronic Circuits Homework 1 Due Friday January 25, 2008Document1 pageECE 442 Electronic Circuits Homework 1 Due Friday January 25, 2008Đỗ Minh QuốcNo ratings yet
- Sumatera-Jawa Transmission ProjectDocument7 pagesSumatera-Jawa Transmission ProjectSingal SihombingNo ratings yet
- Vintage Lenses 20211124 153207Document6 pagesVintage Lenses 20211124 153207Jiang Hao (seiend)No ratings yet
- Safety Valve - 118CSS SpecificationDocument2 pagesSafety Valve - 118CSS SpecificationManuel Pimentel Del Campo100% (1)
- Wall Mount EnclosureDocument8 pagesWall Mount Enclosurejfmg1971No ratings yet
- A Review On BIM-based Automated Code Compliance Checking SystemDocument6 pagesA Review On BIM-based Automated Code Compliance Checking SystemKavish BhagwatNo ratings yet
- McKinsey Life Insurance 2.0Document52 pagesMcKinsey Life Insurance 2.0Moushumi DharNo ratings yet
- Chemistry Syllabus New Curriculum - pdf-2Document53 pagesChemistry Syllabus New Curriculum - pdf-2donNo ratings yet
- Topic 5: Darkroom Conditions For Radiographic Facilities: X-Ray Facility TipsDocument3 pagesTopic 5: Darkroom Conditions For Radiographic Facilities: X-Ray Facility TipsAmrina RosyadaNo ratings yet
- 10 1007@BF02191557Document10 pages10 1007@BF02191557Sol LakosNo ratings yet
- Hi Focus f152 HBDocument4 pagesHi Focus f152 HBAna Bogdanovic GagiNo ratings yet
- 39 Integration Using Algebraic Substitutions PDFDocument3 pages39 Integration Using Algebraic Substitutions PDFMelissaNo ratings yet
- A Level NEA Guide To Titles and Proposal FormsDocument20 pagesA Level NEA Guide To Titles and Proposal FormsAsdfgh AsdfghjkNo ratings yet
- Lab 3 Ee480Document1 pageLab 3 Ee480Kuro ShiroNo ratings yet
- Markets and DestinationDocument55 pagesMarkets and DestinationJorim Sumangid100% (1)
- 4 - Classical Management 2Document64 pages4 - Classical Management 2Prof. Maseera PatelNo ratings yet
- Super Star Group: Subject: Work Order For Supply of Switch With Box SingleDocument29 pagesSuper Star Group: Subject: Work Order For Supply of Switch With Box SingleAntora HoqueNo ratings yet
- CH 5Document21 pagesCH 5Yosef KetemaNo ratings yet
- "I Am Not Complaining"-Ambivalence Construct in Schizoid Personality DisorderDocument22 pages"I Am Not Complaining"-Ambivalence Construct in Schizoid Personality DisorderinsildaNo ratings yet
- Microprocessor Counter and Time DelayDocument10 pagesMicroprocessor Counter and Time DelaySamir KumarNo ratings yet
- Tunneling Technologies: Centre of Expertise For Equipment TechnologyDocument5 pagesTunneling Technologies: Centre of Expertise For Equipment Technologymoin4cuetNo ratings yet