You might also like
- Oxygen Saturation (If Available) : IagnosisDocument3 pagesOxygen Saturation (If Available) : Iagnosisrezairfan221No ratings yet
- Rare and Interesting Cases in Pulmonary MedicineFrom EverandRare and Interesting Cases in Pulmonary MedicineRating: 4 out of 5 stars4/5 (1)
- Lower Respiratory (Autosaved)Document58 pagesLower Respiratory (Autosaved)VIVEK DHADYANNo ratings yet
- North Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaFrom EverandNorth Carolina Children’s Global Health Handbook: A Pediatrician’s Guide to Integrating IMCI Guidelines in Sub-Saharan AfricaErica C. BjornstadNo ratings yet
- Respiratory Distress in Newborn: Presented By: Dr. Walaa MousaDocument74 pagesRespiratory Distress in Newborn: Presented By: Dr. Walaa MousasalamredNo ratings yet
- Neonatal SepsisDocument20 pagesNeonatal SepsisNilanduniNo ratings yet
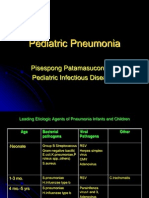
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDocument39 pagesPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNo ratings yet
- Sepsis in PediatricsDocument48 pagesSepsis in PediatricsCecile Maramba-LazarteNo ratings yet
- PneumoniaDocument26 pagesPneumonialovelots1234No ratings yet
- PneumoniaDocument38 pagesPneumoniaAzhar GhoriNo ratings yet
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisDocument40 pagesKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihNo ratings yet
- Pediatric Critical CareDocument3 pagesPediatric Critical CareRem AlfelorNo ratings yet
- Common Diseases of NewbornDocument162 pagesCommon Diseases of NewbornMichelle ThereseNo ratings yet
- Pneumonia 1Document31 pagesPneumonia 1Parushhni NandhagopalNo ratings yet
- W1 L3 Wheezy InfantsDocument36 pagesW1 L3 Wheezy InfantsAnas FikriNo ratings yet
- Paediatric-Chronic CoughDocument66 pagesPaediatric-Chronic CoughIzyan NadhirahNo ratings yet
- 3.pulmonary Alterations - Part 2Document37 pages3.pulmonary Alterations - Part 2Rawan AlotaibiNo ratings yet
- Cap, Hap, VapDocument63 pagesCap, Hap, Vapbekbekk cabahugNo ratings yet
- W1 L2 PneumoniaDocument57 pagesW1 L2 PneumoniaAnas FikriNo ratings yet
- Community Acquired PneumoniaDocument9 pagesCommunity Acquired PneumoniaSuzette Rae TateNo ratings yet
- P E: R F: Aediatric Mergencies Espiratory AilureDocument38 pagesP E: R F: Aediatric Mergencies Espiratory AilureAfiqah So JasmiNo ratings yet
- 30 PneumoniaDocument3 pages30 PneumoniaChameera JayasankaNo ratings yet
- Paeds Case 1 - Writeup-1Document14 pagesPaeds Case 1 - Writeup-1Shakshi RainaNo ratings yet
- Neonatal Respiratory DistressDocument59 pagesNeonatal Respiratory DistressMohamad Saleh100% (7)
- ShockDocument34 pagesShockAnthon Kyle TropezadoNo ratings yet
- Transient Tachypnea of The NewbornDocument4 pagesTransient Tachypnea of The NewbornKhaled SghaierNo ratings yet
- Respiratory Distress Syndrome LapkasDocument49 pagesRespiratory Distress Syndrome LapkasThamarai SomuNo ratings yet
- Community-Acquired Pneumonia: Joanna M. Delaney, D.O. Georgetown University / Providence Hospital June 8, 2007Document38 pagesCommunity-Acquired Pneumonia: Joanna M. Delaney, D.O. Georgetown University / Providence Hospital June 8, 2007shiean06No ratings yet
- Pediatrics L6: Dodo AgladzeDocument32 pagesPediatrics L6: Dodo AgladzeluckyNo ratings yet
- Acute Lower Respiratory Tract Infection (ALRTI)Document43 pagesAcute Lower Respiratory Tract Infection (ALRTI)yosephNo ratings yet
- Topic 2. Dyspnea. Complecated Pneumonia in Children. - ShortDocument69 pagesTopic 2. Dyspnea. Complecated Pneumonia in Children. - ShortIbtissame BadadNo ratings yet
- Pediatric PneumoniaDocument58 pagesPediatric PneumoniaJohn Christopher LucesNo ratings yet
- Pneumonia PDFDocument68 pagesPneumonia PDFfatiniNo ratings yet
- Bronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDDocument37 pagesBronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDYuusuf MubarikNo ratings yet
- AARC Clinical Practice GuidelineDocument23 pagesAARC Clinical Practice GuidelineModsom OouiNo ratings yet
- Critically Ill PatientDocument31 pagesCritically Ill PatientSameh Aziz100% (1)
- RESPIRATORY DISORDERS (Abdurahman S)Document19 pagesRESPIRATORY DISORDERS (Abdurahman S)Rahmat MuliaNo ratings yet
- Dengue: (Mosquito Borne)Document45 pagesDengue: (Mosquito Borne)Sibi PalanisamyNo ratings yet
- Topic Respiratory Distress in NewbornDocument45 pagesTopic Respiratory Distress in NewbornICETNPNo ratings yet
- Clinical Presentation On Child With Neonatal SepsisDocument37 pagesClinical Presentation On Child With Neonatal SepsisSREEDEVI T SURESHNo ratings yet
- Respiratory DistressDocument6 pagesRespiratory DistressChyntia Vini A RNo ratings yet
- Shelly PneumoniaDocument34 pagesShelly PneumoniaFandhyy H. SetiawanNo ratings yet
- ICU Assessment Powerpoit Tuts1Document25 pagesICU Assessment Powerpoit Tuts1Sharom SalasNo ratings yet
- PNEUMONIA - The Evil DiseaseDocument29 pagesPNEUMONIA - The Evil Diseasesitesh009No ratings yet
- Exam in IccuDocument15 pagesExam in IccuDewi AmeliaNo ratings yet
- 6.2 Sespsis TargovisteDocument50 pages6.2 Sespsis TargovisteIna MarinNo ratings yet
- Paul Kolesnyk: Cold-Practical Approach of Family DoctorDocument34 pagesPaul Kolesnyk: Cold-Practical Approach of Family Doctoranon_20012817No ratings yet
- Draft PaedDocument80 pagesDraft PaedEu May KhorNo ratings yet
- DengueDocument36 pagesDengueMohd Alfian Awang Ku LekNo ratings yet
- Pneumonia AlgorithmDocument3 pagesPneumonia AlgorithmBien ChuNo ratings yet
- Respiratory Distress in NewbornDocument32 pagesRespiratory Distress in NewbornCharu KalraNo ratings yet
- Nursing Care With PenumoniaDocument44 pagesNursing Care With PenumoniaFahmi SyarifNo ratings yet
- Presentation By:-Capt Narendra Sarlam MH GwaliorDocument66 pagesPresentation By:-Capt Narendra Sarlam MH Gwalioryash shrivastavaNo ratings yet
- Enteroviruses: Prepared By: Eriwan Osman Daban Azad Dastan Hadi Omer Ahmed Zanyar QadrDocument33 pagesEnteroviruses: Prepared By: Eriwan Osman Daban Azad Dastan Hadi Omer Ahmed Zanyar QadrDastan HadiNo ratings yet
- Medical Surgical Nursing - RespiratoryDocument15 pagesMedical Surgical Nursing - RespiratoryChristian Esteves75% (4)
- San Lazaro Question Bank SouthPark 2Document9 pagesSan Lazaro Question Bank SouthPark 2Kenneth MiguelNo ratings yet
- Puerperal SepsisDocument11 pagesPuerperal SepsisLana LocoNo ratings yet
- Acute Exacerbation of CopdDocument28 pagesAcute Exacerbation of CopdMohd RafiNo ratings yet
- PCAP Report ClerkshipDocument54 pagesPCAP Report ClerkshipMichelleAquinoSuzukiNo ratings yet
- Drug AllergyDocument39 pagesDrug AllergyluckyNo ratings yet
- AngioedemaDocument26 pagesAngioedemaluckyNo ratings yet
- Anaphylaxis 2Document34 pagesAnaphylaxis 2luckyNo ratings yet
- Moduli Asthma 2Document24 pagesModuli Asthma 2luckyNo ratings yet
- Urticaria LesionsDocument9 pagesUrticaria LesionsluckyNo ratings yet
- Pediatrics L6: Dodo AgladzeDocument32 pagesPediatrics L6: Dodo AgladzeluckyNo ratings yet
- Ped 4Document28 pagesPed 4luckyNo ratings yet
- Hemostasis: Primary and Secondary HemostasisDocument52 pagesHemostasis: Primary and Secondary HemostasisluckyNo ratings yet
- Pediatrics L3: Dodo AgladzeDocument28 pagesPediatrics L3: Dodo AgladzeluckyNo ratings yet
- Pediatrics L2: Dodo AgladzeDocument35 pagesPediatrics L2: Dodo AgladzeluckyNo ratings yet
- InflammationmedDocument83 pagesInflammationmedluckyNo ratings yet
- MenopausepptDocument24 pagesMenopausepptluckyNo ratings yet
- Introduction To LeukemiaDocument51 pagesIntroduction To LeukemiaMeldiana100% (1)
- BrainstemDocument16 pagesBrainstemluckyNo ratings yet
- Motor System: G. Arveladze N. MalashkhiaDocument17 pagesMotor System: G. Arveladze N. MalashkhialuckyNo ratings yet
- Optical SystemDocument23 pagesOptical SystemluckyNo ratings yet
- Headache TypesDocument29 pagesHeadache TypesluckyNo ratings yet
- GingivaDocument69 pagesGingivaluckyNo ratings yet
- Motor System: G. Arveladze N. MalashkhiaDocument17 pagesMotor System: G. Arveladze N. MalashkhialuckyNo ratings yet
- Trigeminal NerveDocument11 pagesTrigeminal NerveluckyNo ratings yet
- Autonomic N.SDocument12 pagesAutonomic N.SluckyNo ratings yet
- Anatomy of The EyeballDocument54 pagesAnatomy of The EyeballluckyNo ratings yet
- Trigeminal NerveDocument11 pagesTrigeminal NerveluckyNo ratings yet
- Motor System: G. Arveladze N. MalashkhiaDocument17 pagesMotor System: G. Arveladze N. MalashkhialuckyNo ratings yet
- Autonomic N.SDocument12 pagesAutonomic N.SluckyNo ratings yet
- Ocular Examination and Imaging TechniqueDocument33 pagesOcular Examination and Imaging TechniqueluckyNo ratings yet
- Facial Nerve (CN VII) and Nervus IntermediusDocument8 pagesFacial Nerve (CN VII) and Nervus IntermediusluckyNo ratings yet
- Anatomy of The EyeballDocument54 pagesAnatomy of The EyeballluckyNo ratings yet
- Motor System: G. Arveladze N. MalashkhiaDocument17 pagesMotor System: G. Arveladze N. MalashkhialuckyNo ratings yet
- Unit Plan - Yr 9 Vis ArtDocument5 pagesUnit Plan - Yr 9 Vis Artapi-333348168No ratings yet
- Too Early! by Anton Pavlovich ChekhovDocument4 pagesToo Early! by Anton Pavlovich Chekhovapi-19787590No ratings yet
- Air Quality StandardsDocument2 pagesAir Quality StandardsJanmejaya BarikNo ratings yet
- Sheet - PDF 3Document4 pagesSheet - PDF 3Nazar JabbarNo ratings yet
- Organizational Behavior Exam 2 Practice QuestionsDocument1 pageOrganizational Behavior Exam 2 Practice QuestionsSydney EverettNo ratings yet
- Assignment-3: Marketing Management (MGT201)Document6 pagesAssignment-3: Marketing Management (MGT201)Rizza L. MacarandanNo ratings yet
- Mat210 LectureNotes 1Document7 pagesMat210 LectureNotes 1Franch Maverick Arellano LorillaNo ratings yet
- Kuka Interbus InterfaceDocument11 pagesKuka Interbus InterfaceAnonymous Zh6p3ENo ratings yet
- If Else ExercisesDocument5 pagesIf Else ExercisesHoney Jean PerezNo ratings yet
- Cement Grouted Rock BoltsDocument28 pagesCement Grouted Rock BoltsBhaskar ReddyNo ratings yet
- Airport Lounges Industry-Report-Frost-SullivanDocument112 pagesAirport Lounges Industry-Report-Frost-SullivansandeepNo ratings yet
- Eating Well: Snacks For 1-4 Year OldsDocument42 pagesEating Well: Snacks For 1-4 Year OldsAndreea AndreiNo ratings yet
- SIP Debugging Commands Overview - Cisco CommunityDocument5 pagesSIP Debugging Commands Overview - Cisco CommunitysenthilNo ratings yet
- h4 History of India Ad 1526 - Ad 1707Document2 pagesh4 History of India Ad 1526 - Ad 1707Baddela ReddyNo ratings yet
- Functional Plant Manager 2. Geographical Vice PresidentDocument5 pagesFunctional Plant Manager 2. Geographical Vice PresidentVic FranciscoNo ratings yet
- AQA Power and Conflict GCSE Revision Guide LADocument49 pagesAQA Power and Conflict GCSE Revision Guide LAderaw11557No ratings yet
- Q1 WK 2 To 3 Las Fabm2 Kate DionisioDocument8 pagesQ1 WK 2 To 3 Las Fabm2 Kate DionisioFunji BuhatNo ratings yet
- Pricelist LV Siemens 2019 PDFDocument96 pagesPricelist LV Siemens 2019 PDFBerlianiNo ratings yet
- HLSS 310 Critical Infrastructure ProtectionDocument12 pagesHLSS 310 Critical Infrastructure ProtectionMoffat HarounNo ratings yet
- The Light BulbDocument6 pagesThe Light Bulbapi-244765407No ratings yet
- Discovering JerusalemDocument134 pagesDiscovering JerusalemDzhel DezjayNo ratings yet
- CM658 Time - MNGT - 10 - Getting Know The Class - NewNormDocument12 pagesCM658 Time - MNGT - 10 - Getting Know The Class - NewNormLee BañezNo ratings yet
- Marking Scheme According To AIDocument2 pagesMarking Scheme According To AIAbdul RehmanNo ratings yet
- Bubbles in Transformer Oil Dynamic Behavior Internal Discharge and Triggered Liquid BreakdownDocument9 pagesBubbles in Transformer Oil Dynamic Behavior Internal Discharge and Triggered Liquid BreakdownMuhammad Irfan NazhmiNo ratings yet
- A 268 - A 268M - 01 Qti2oc0wmq - PDFDocument6 pagesA 268 - A 268M - 01 Qti2oc0wmq - PDFMan98No ratings yet
- Management From RamayanaDocument14 pagesManagement From Ramayanasaaket batchuNo ratings yet
- Emmanuel John MangahisDocument15 pagesEmmanuel John MangahisEmmanuel MangahisNo ratings yet
- Pengaruh PH Ekstraksi Terhadap Rendemen, Sifat Fisiko-Kimia Dan Fungsional Konsentrat Protein KACANG GUDE (Cajanus Cajan (L.) Millsp.)Document11 pagesPengaruh PH Ekstraksi Terhadap Rendemen, Sifat Fisiko-Kimia Dan Fungsional Konsentrat Protein KACANG GUDE (Cajanus Cajan (L.) Millsp.)Rezaa RezNo ratings yet
- ADCD LowDocument8 pagesADCD LowrahulmultivisionNo ratings yet
- Indian Space Research OrganisationDocument5 pagesIndian Space Research OrganisationGarima GoyalNo ratings yet