You might also like
- Ear ExaminationDocument47 pagesEar ExaminationHarshit Bhardwaj100% (4)
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- ENT - Clinical NotesDocument114 pagesENT - Clinical NotesTANINo ratings yet
- Basic Physical Examination in ENT PDFDocument44 pagesBasic Physical Examination in ENT PDFJayricDepalobosNo ratings yet
- Basic Physical Examination in ENTDocument44 pagesBasic Physical Examination in ENTKIWANUKA GEORGE100% (1)
- Endotracheal IntubationDocument43 pagesEndotracheal IntubationBishow100% (1)
- Ent ExaminationDocument85 pagesEnt ExaminationDevi Yusfita100% (1)
- EntDocument105 pagesEntNikhil KumarNo ratings yet
- EntDocument32 pagesEntaini natasha100% (3)
- Ent History Taking and Examination-1Document16 pagesEnt History Taking and Examination-1Jyotirmayee100% (5)
- Ent Eye Osce Totes - YJDocument31 pagesEnt Eye Osce Totes - YJanon_373532435No ratings yet
- Health Assessment EarsDocument42 pagesHealth Assessment EarsMary Jane M. MorenoNo ratings yet
- Manajemen AirwayDocument91 pagesManajemen AirwayAnonymous niVHtxvPNo ratings yet
- ENT Clinical Skill: Dr. Pulo R S Banjarnahor, SP THT-KL Dr. Reno H Kelan, SP - THT-KLDocument80 pagesENT Clinical Skill: Dr. Pulo R S Banjarnahor, SP THT-KL Dr. Reno H Kelan, SP - THT-KLDavidVictoriousLukasNo ratings yet
- Modul Anatomi Blok 11Document40 pagesModul Anatomi Blok 11AyuNo ratings yet
- Introduction To Ent and Basic ENT ExaminationDocument34 pagesIntroduction To Ent and Basic ENT Examinationalmazmulu76No ratings yet
- The Ear History & Hearing TestsDocument5 pagesThe Ear History & Hearing TestsNoelle Grace Ulep BaromanNo ratings yet
- Assessment of The Ear, Nose and ThroatDocument40 pagesAssessment of The Ear, Nose and Throatsnickers_j100% (3)
- Approach To Examination of ENT DisordersDocument39 pagesApproach To Examination of ENT DisordersMohammad SaifullahNo ratings yet
- Assessment of EarDocument43 pagesAssessment of Earraima ayazNo ratings yet
- Ent and OptalmologyDocument138 pagesEnt and OptalmologyFan Eli100% (3)
- Aj Anatomy - and - Physiology - of - Nose - & - Paranasal - SinusDocument117 pagesAj Anatomy - and - Physiology - of - Nose - & - Paranasal - SinusTradigrade PukarNo ratings yet
- ENT Physical Examination (Head & Neck, Ear, Nose and Throat) Physical ExaminationDocument78 pagesENT Physical Examination (Head & Neck, Ear, Nose and Throat) Physical ExaminationMojahid AliNo ratings yet
- Assessing Nose and Sinuses2Document36 pagesAssessing Nose and Sinuses2Hannah Vuelta100% (2)
- ENT Case Proforma-EarDocument8 pagesENT Case Proforma-EarGaneshNo ratings yet
- Otolaryngology For Medical StudentsDocument112 pagesOtolaryngology For Medical StudentsDrsreeram ValluriNo ratings yet
- Pemeriksaan Fisik THTDocument83 pagesPemeriksaan Fisik THTClara ReginaNo ratings yet
- Nose, Mouth, ThroutDocument78 pagesNose, Mouth, ThroutChaudhary AjayNo ratings yet
- Examination of Ear - Nose and - ThroatDocument77 pagesExamination of Ear - Nose and - Throatapi-19641337100% (3)
- Presentasi Jurnal LaryngoceleDocument13 pagesPresentasi Jurnal LaryngoceleTiara Rachmaputeri AriantoNo ratings yet
- Tests of Eustachean Tube FunctionDocument3 pagesTests of Eustachean Tube FunctionAnish RajNo ratings yet
- ENT Previous Year QuestionsDocument13 pagesENT Previous Year QuestionsKoki AlagarNo ratings yet
- Examination of NoseDocument63 pagesExamination of NoseDr Sravya M VNo ratings yet
- THT Examination: Fitria Amanda N 101 14 019Document15 pagesTHT Examination: Fitria Amanda N 101 14 019Fitria AmandaNo ratings yet
- 13 Otoscope UseDocument61 pages13 Otoscope UseJayakumar D Swamy0% (1)
- History and Examination in EntDocument71 pagesHistory and Examination in EntMuhammad Naquib AliNo ratings yet
- HEENT, Neuro, Pulmonary, Cardiovascular and Abdominal ExamsDocument100 pagesHEENT, Neuro, Pulmonary, Cardiovascular and Abdominal ExamsMonica J Ortiz PereiraNo ratings yet
- ENT Short Cases Records & OSCE Questions: 1 EditionDocument15 pagesENT Short Cases Records & OSCE Questions: 1 EditionSaya MenangNo ratings yet
- 7 - Ear 1Document40 pages7 - Ear 1Touseeq ManzoorNo ratings yet
- Foreign Bodies of the Aerodigestive TractDocument70 pagesForeign Bodies of the Aerodigestive TractHòa NguyễnNo ratings yet
- Clinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Document30 pagesClinical Examination of The Ear, Nose and Throat: Dave Pothier ST Mary's 2003Ekambaram TrmNo ratings yet
- The Anatomy and Rhinoscopy of the NoseDocument15 pagesThe Anatomy and Rhinoscopy of the NoseMadalina DutanNo ratings yet
- Respiratory Tract Anatomy and PhysiologyDocument37 pagesRespiratory Tract Anatomy and PhysiologyJuwitaNo ratings yet
- Rinne Test: Screening for Conductive Hearing LossDocument3 pagesRinne Test: Screening for Conductive Hearing LossSuranewNo ratings yet
- Lecture 1 Ent.Document60 pagesLecture 1 Ent.kiprotich weldonNo ratings yet
- Otolaryngology: (Otolaryngology Head and Neck Surgery)Document65 pagesOtolaryngology: (Otolaryngology Head and Neck Surgery)EINSTEIN2DNo ratings yet
- ENT Notes CrakDocument52 pagesENT Notes CrakGrant KimNo ratings yet
- Introducere 1Document11 pagesIntroducere 1Victor EnachiNo ratings yet
- ENT MCQforstudents AnswersDocument30 pagesENT MCQforstudents AnswersOlaNo ratings yet
- ENT Concept BookDocument177 pagesENT Concept BookPrincyNo ratings yet
- Assessment and Management ofDocument123 pagesAssessment and Management ofshekinahNo ratings yet
- EntDocument176 pagesEntLucian TerbeaNo ratings yet
- Penatalaksanaan Jalan NapasDocument42 pagesPenatalaksanaan Jalan NapasFANI RUDIYANTI 1No ratings yet
- ENT EquipmentDocument14 pagesENT EquipmentCarlous Shuga ChadwickNo ratings yet
- 2 Throat ExaminationDocument15 pages2 Throat ExaminationMariam QaisNo ratings yet
- Review For ENT (2008 Batch)Document9 pagesReview For ENT (2008 Batch)HaslinNo ratings yet
- Ear, Nose, Throat Health AssessmentDocument11 pagesEar, Nose, Throat Health AssessmentJaseel Muhammed BNo ratings yet
- Unit-8-Ear, Nose, Mouth, Sinus and Pharynx ExaminationDocument104 pagesUnit-8-Ear, Nose, Mouth, Sinus and Pharynx ExaminationMinlik-alew Dejenie100% (5)
- Nose and PNSDocument58 pagesNose and PNSChekole AdaneNo ratings yet
- Types of Stroke and Their SymptomsDocument30 pagesTypes of Stroke and Their SymptomsRizky PebryanNo ratings yet
- Refraction: DR Intan Dwi Rahayu SPMDocument52 pagesRefraction: DR Intan Dwi Rahayu SPMlaksonoNo ratings yet
- Hidung TersumbatDocument13 pagesHidung TersumbatRizky PebryanNo ratings yet
- LEVEL OF PREVENTION-dr - WITRIDocument10 pagesLEVEL OF PREVENTION-dr - WITRIHirotaka KitabatakeNo ratings yet
- RetinaDocument57 pagesRetinaRizky PebryanNo ratings yet
- Examination of The Ears, Nose, Throat, and NeckDocument85 pagesExamination of The Ears, Nose, Throat, and NeckRizky PebryanNo ratings yet
- 3.3 Neurosensory Disorders Mikrobiologi 2018-2019 RRDocument202 pages3.3 Neurosensory Disorders Mikrobiologi 2018-2019 RRRizky PebryanNo ratings yet
- Anatomi - FisiologiDocument22 pagesAnatomi - FisiologiRizky PebryanNo ratings yet
- Structure & Function of Gene and GenomeDocument53 pagesStructure & Function of Gene and GenomeGhina JD100% (1)
- Hospital EpidemiologymiologyDocument98 pagesHospital EpidemiologymiologyRizky PebryanNo ratings yet
- Divisi Fisiologi FK Unswagati Divisi Fisiologi FK UnswagatiDocument53 pagesDivisi Fisiologi FK Unswagati Divisi Fisiologi FK UnswagatiRizky PebryanNo ratings yet
- Pengukuran Kemampuan Belajar Mandiri Pada Mahasiswa Pendidikan Profesi DokterDocument19 pagesPengukuran Kemampuan Belajar Mandiri Pada Mahasiswa Pendidikan Profesi DokterRizky PebryanNo ratings yet
- Cot 1 Detailed Lesson Plan in Science 10Document3 pagesCot 1 Detailed Lesson Plan in Science 10Arlen FuentebellaNo ratings yet
- Chapter 21 I Variations ENHANCEDocument21 pagesChapter 21 I Variations ENHANCENorazah AhmadNo ratings yet
- 74HCT00Document8 pages74HCT00Sadikul FuadNo ratings yet
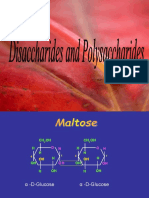
- Disaccharides and PolysaccharidesDocument17 pagesDisaccharides and PolysaccharidesAarthi shreeNo ratings yet
- Levitator Ino - InoDocument2 pagesLevitator Ino - InoSUBHANKAR BAGNo ratings yet
- Installation Manual MSP DUCT - SLIM DUCT PDFDocument31 pagesInstallation Manual MSP DUCT - SLIM DUCT PDFutaiuliancatalinNo ratings yet
- The Philosophy of Composition (1846)Document20 pagesThe Philosophy of Composition (1846)Denise CoronelNo ratings yet
- Al-Qawlul Mufeed: Backbiting and Its Impact On SocietyDocument2 pagesAl-Qawlul Mufeed: Backbiting and Its Impact On SocietyMountainofknowledgeNo ratings yet
- Simple BoxDocument104 pagesSimple BoxTÙNGNo ratings yet
- FulfillerDocument8 pagesFulfillermanojeil1No ratings yet
- From Verse Into A Prose, English Translations of Louis Labe (Gerard Sharpling)Document22 pagesFrom Verse Into A Prose, English Translations of Louis Labe (Gerard Sharpling)billypilgrim_sfeNo ratings yet
- TB170LSDocument4 pagesTB170LSDary ArroyoNo ratings yet
- Body Condition Scoring of Dairy Cattle A Review - 2 PDFDocument8 pagesBody Condition Scoring of Dairy Cattle A Review - 2 PDFfrankyNo ratings yet
- Philippine Poetry:: It's Form, Language, and SpeechDocument12 pagesPhilippine Poetry:: It's Form, Language, and SpeechRis AsibronNo ratings yet
- Shwebo District ADocument280 pagesShwebo District AKyaw MaungNo ratings yet
- Xist PDFDocument2 pagesXist PDFAgustin Gago LopezNo ratings yet
- Country/Airport City Laboratory: AfghanistanDocument25 pagesCountry/Airport City Laboratory: AfghanistanLudovic DumitruNo ratings yet
- The Most Efficient and Effective Ways To Address New Literacies FDocument61 pagesThe Most Efficient and Effective Ways To Address New Literacies FAlpha MoontonNo ratings yet
- Postgraduate Prospectus 2021: World ChangersDocument35 pagesPostgraduate Prospectus 2021: World ChangersSKNo ratings yet
- Section10 - POST-DRILLING ACTIVITIESDocument16 pagesSection10 - POST-DRILLING ACTIVITIESMohamed ElshoraNo ratings yet
- XETEC 4g300 / 4g600Document6 pagesXETEC 4g300 / 4g600Harun ARIKNo ratings yet
- Well Plug and Abandonment Using HwuDocument1 pageWell Plug and Abandonment Using HwuJuan Pablo CassanelliNo ratings yet
- A2 Unit 4 Academic Skills Plus LessonDocument2 pagesA2 Unit 4 Academic Skills Plus LessonJanaNo ratings yet
- VachanamruthaDocument5 pagesVachanamruthaypraviNo ratings yet
- The Man Who Married A Hen, Stories of A Zambian SchoolboyDocument78 pagesThe Man Who Married A Hen, Stories of A Zambian SchoolboyGerard StoutNo ratings yet
- Jitante Stotram v4 PDFDocument71 pagesJitante Stotram v4 PDFRamadevaNo ratings yet
- Oxford Classical Dictionary AbbreviationsDocument9 pagesOxford Classical Dictionary AbbreviationsScotch_Nights_Order0% (2)
- Spent Caustic Recycle at Farleigh MillDocument9 pagesSpent Caustic Recycle at Farleigh MillyamakunNo ratings yet
- Invoice Being Charged Sued If or Violation Has This in Wrongful - RightfulDocument67 pagesInvoice Being Charged Sued If or Violation Has This in Wrongful - RightfulSteven SchoferNo ratings yet
- The Law of DemandDocument13 pagesThe Law of DemandAngelique MancillaNo ratings yet