You might also like
- ENT MCQforstudents AnswersDocument30 pagesENT MCQforstudents AnswersOlaNo ratings yet
- Maxillary Sinus Anatomy and Oroantral FistulaDocument26 pagesMaxillary Sinus Anatomy and Oroantral FistulaRobins DhakalNo ratings yet
- Adenoid Hypertrophy and Serous Otitis MediaDocument31 pagesAdenoid Hypertrophy and Serous Otitis MediaFatima JamshaidNo ratings yet
- Ear, Nose and Throat ConditionsDocument10 pagesEar, Nose and Throat ConditionsSaileekitha AjamoniNo ratings yet
- Tests of Eustachean Tube FunctionDocument3 pagesTests of Eustachean Tube FunctionAnish RajNo ratings yet
- EXTERNAL EAR DISORDERS AND DEFORMITIESDocument48 pagesEXTERNAL EAR DISORDERS AND DEFORMITIEShemaanandhyNo ratings yet
- مراجعة الأوسكىDocument238 pagesمراجعة الأوسكىHala BahaaNo ratings yet
- Nasal Obstruction: Nitha K 2nd Year MSC NursingDocument65 pagesNasal Obstruction: Nitha K 2nd Year MSC NursingNITHA KNo ratings yet
- diagnosis-of-ent-disorders-you-make-the-callDocument137 pagesdiagnosis-of-ent-disorders-you-make-the-callsaifsaffa2No ratings yet
- ORL Interns NotesDocument15 pagesORL Interns NotesDaphne Ongbit JaritoNo ratings yet
- Ears&MouthDocument76 pagesEars&Mouthrichelley08No ratings yet
- Ear ExaminationDocument47 pagesEar ExaminationHarshit Bhardwaj100% (4)
- HEENT Nursing AssessmentDocument12 pagesHEENT Nursing AssessmentMelissa Aina Mohd Yusof100% (1)
- Ear Anatomy and External Canal ConditionsDocument39 pagesEar Anatomy and External Canal ConditionsMahmoud Abu Al Amrain100% (1)
- Common Ent EmergenciesDocument65 pagesCommon Ent EmergenciesferaNo ratings yet
- Acute Otitis MediaDocument16 pagesAcute Otitis Mediaadrianne18sNo ratings yet
- 12 Congenital Lesions of Larynx and Evaluation of StridorDocument77 pages12 Congenital Lesions of Larynx and Evaluation of StridorAbhishek ShahNo ratings yet
- RAJIV DHAWAN ENT FMG RR Watermark Final Corrected 09.11.23Document69 pagesRAJIV DHAWAN ENT FMG RR Watermark Final Corrected 09.11.23Wahib ZaidiNo ratings yet
- 4-Larynx. Cong&trauma of LarynxDocument26 pages4-Larynx. Cong&trauma of LarynxislamNo ratings yet
- Role of ENT Specialist in Treating Speech & Voice DefectsDocument69 pagesRole of ENT Specialist in Treating Speech & Voice DefectsBalakrishnan DoraisamiNo ratings yet
- A. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthDocument6 pagesA. Nasal Symptoms 1. Nasal Obstruction Is The Commonest Symptom. - This Leads To MouthRubi MeeajanNo ratings yet
- Review For ENT (2008 Batch)Document9 pagesReview For ENT (2008 Batch)HaslinNo ratings yet
- Basic Physical Examination in ENTDocument44 pagesBasic Physical Examination in ENTKIWANUKA GEORGE100% (1)
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- EntDocument32 pagesEntaini natasha100% (3)
- Ostrower Preauricular Cysts, Pits, and Fissures - Practice Essentials, Epidemiology, EtiologyDocument8 pagesOstrower Preauricular Cysts, Pits, and Fissures - Practice Essentials, Epidemiology, EtiologyAndre HawkNo ratings yet
- Anatomy Head Neck EMRCS MCQDocument23 pagesAnatomy Head Neck EMRCS MCQTowhid HasanNo ratings yet
- 중이염 Otitis MediaDocument213 pages중이염 Otitis MediaChangho LeeNo ratings yet
- Hearing Impairment by Nyanga KeyDocument4 pagesHearing Impairment by Nyanga KeyMbuyoti KanyataNo ratings yet
- Congenital Ear AnomaliesDocument28 pagesCongenital Ear AnomaliesSacad SuleimanNo ratings yet
- ENT Emergency PresentationDocument135 pagesENT Emergency PresentationshahiruddinNo ratings yet
- ENTDocument51 pagesENTBryan Paul Ramirez100% (1)
- OtalgiaDocument57 pagesOtalgiaKamal-Eldin Ahmed Abou-ElhamdNo ratings yet
- Common Ent Emergencies 24126Document64 pagesCommon Ent Emergencies 24126Krittin NaravejsakulNo ratings yet
- Hearing Loss in Children - Etiology - UpToDateDocument39 pagesHearing Loss in Children - Etiology - UpToDateAlexander AdrielNo ratings yet
- Eardrum Repair Surgery DefinitionDocument4 pagesEardrum Repair Surgery DefinitionMelly Selvia ANo ratings yet
- ENTDocument40 pagesENTwhoosh2008No ratings yet
- Preauricular Sinus and Its ManagmentDocument12 pagesPreauricular Sinus and Its ManagmentDr. T. Balasubramanian100% (7)
- LMR Ent - Nose and Paransal SinusesDocument7 pagesLMR Ent - Nose and Paransal SinusesYuku BabyNo ratings yet
- CSOM Retroauricular FistulaDocument154 pagesCSOM Retroauricular FistulaM.rizki DestiantoroNo ratings yet
- Ear Assessment 4Document49 pagesEar Assessment 4Feven AbrahamNo ratings yet
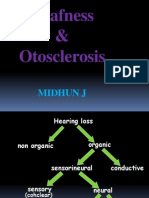
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- Congenital Malformations of Temporal Bone: by Dr. T. Balasubramanian M.S. D.L.ODocument16 pagesCongenital Malformations of Temporal Bone: by Dr. T. Balasubramanian M.S. D.L.OIvan DarioNo ratings yet
- Nasal Obstruction: Meng JuanDocument36 pagesNasal Obstruction: Meng JuanReshma VasuNo ratings yet
- ENT SGD 1 Clinical History and ENT Physical ExaminationDocument51 pagesENT SGD 1 Clinical History and ENT Physical ExaminationEmerson QuimbaNo ratings yet
- Revision Note - 1 - ENT NuggetsDocument4 pagesRevision Note - 1 - ENT NuggetsNicNo ratings yet
- Tamil Nadu DR MGR Medical University ENT MBBS Prefinal Feb 2009 Question Paper With SolutionDocument21 pagesTamil Nadu DR MGR Medical University ENT MBBS Prefinal Feb 2009 Question Paper With SolutionDr. T. BalasubramanianNo ratings yet
- Guide to Laryngoscopy Exam of the Voice BoxDocument3 pagesGuide to Laryngoscopy Exam of the Voice BoxShazNo ratings yet
- The EarDocument59 pagesThe EarJasmin Jacob100% (5)
- External Ear Functions CMDocument6 pagesExternal Ear Functions CMJoe RealNo ratings yet
- Girl's Ear Discharge and Hearing Loss Linked to ColdsDocument13 pagesGirl's Ear Discharge and Hearing Loss Linked to ColdsRetno TharraNo ratings yet
- Ear 1, 2Document9 pagesEar 1, 2Nnbbh HggyyNo ratings yet
- Middle Ear Effusion Case FileDocument2 pagesMiddle Ear Effusion Case Filehttps://medical-phd.blogspot.comNo ratings yet
- MGRUniv UGMar07Document32 pagesMGRUniv UGMar07Dr. T. BalasubramanianNo ratings yet
- Examination of Ear - Nose and - ThroatDocument77 pagesExamination of Ear - Nose and - Throatapi-19641337100% (3)
- Congenital MalformationsDocument16 pagesCongenital MalformationsJohn Christopher LucesNo ratings yet
- Pathology of The LarynxDocument17 pagesPathology of The LarynxsallykamareddineNo ratings yet
- 6 +Assessing+Ears+and+NoseDocument55 pages6 +Assessing+Ears+and+Nosejapheth agoncilloNo ratings yet
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Ibuprofen Drug StudyDocument3 pagesIbuprofen Drug StudySeann Loresco100% (2)
- Pharmacology Exams and NotesDocument17 pagesPharmacology Exams and NotesMrz AlzNo ratings yet
- Case Study On Normal Vaginal DeliveryDocument21 pagesCase Study On Normal Vaginal DeliveryPabhat Kumar57% (7)
- Hepatic Lyphoma: Two Cases ReportDocument6 pagesHepatic Lyphoma: Two Cases ReportIJAR JOURNALNo ratings yet
- ICU Sepsis Management GuideDocument139 pagesICU Sepsis Management GuideMuhammad Farid100% (1)
- Managing Health in The Aluminium IndustryDocument346 pagesManaging Health in The Aluminium IndustryWellfro100% (1)
- Bronchodilators Guide for Asthma and COPDDocument5 pagesBronchodilators Guide for Asthma and COPDdeepika kushwahNo ratings yet
- Prostatitis Diagnosis and TreatmentDocument31 pagesProstatitis Diagnosis and TreatmentMuhammad Makki0% (1)
- Beyond Bowels: Understanding Co-existing Symptoms in IBSDocument8 pagesBeyond Bowels: Understanding Co-existing Symptoms in IBSparthibanemails5779No ratings yet
- Sample Death CertificateDocument4 pagesSample Death Certificatenashobo67% (3)
- MCS 200 - 9 - Respiratory SystemDocument49 pagesMCS 200 - 9 - Respiratory SystemYotam MbaoNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Midterm Examination-BiochemDocument10 pagesMidterm Examination-BiochemRhizel Marie Cauilan FariñasNo ratings yet
- Hypoxia - Ischemic EncephalopathyDocument50 pagesHypoxia - Ischemic Encephalopathyapi-19916399No ratings yet
- Aiims Capsule AtfDocument252 pagesAiims Capsule Atfsimrankaur2003studNo ratings yet
- Small Incision CholecystectomyDocument8 pagesSmall Incision CholecystectomyCatalin SavinNo ratings yet
- Selected Differential Diagnosis of Red Eye: Table 1Document3 pagesSelected Differential Diagnosis of Red Eye: Table 1Rian DamayantiNo ratings yet
- Nursing Care of The Patient With Schizophrenia & Psychosis F20Document47 pagesNursing Care of The Patient With Schizophrenia & Psychosis F20nidhi PatelNo ratings yet
- Drug StudyDocument9 pagesDrug StudyKAROL MARIAE LUZ ERESNo ratings yet
- Clinical Practice Guidelines For The Management of DepressionDocument17 pagesClinical Practice Guidelines For The Management of DepressionAnamika SinhaNo ratings yet
- MATERNALDocument14 pagesMATERNALjhenwilliamsNo ratings yet
- GI Drugs: Effects on Vomiting, Diarrhea and ConstipationDocument37 pagesGI Drugs: Effects on Vomiting, Diarrhea and ConstipationRachel CabiguenNo ratings yet
- Anthropometric Measurements and Nutritional AssessmentsDocument14 pagesAnthropometric Measurements and Nutritional AssessmentsSyeda Zainab AbbasNo ratings yet
- Health Assess - Chapter 23 Key TermsDocument3 pagesHealth Assess - Chapter 23 Key TermsAllison Doubek GibsonNo ratings yet
- Pathology ChartsDocument21 pagesPathology Chartspadma maliniNo ratings yet
- Infeksi Tulang Dan Sendi: Preceptor: Dr. Rima Saputri, SP - RadDocument26 pagesInfeksi Tulang Dan Sendi: Preceptor: Dr. Rima Saputri, SP - RadSitti_HazrinaNo ratings yet
- Manage Cellulitis at HomeDocument2 pagesManage Cellulitis at HomeAnonymous 4txA8N8etNo ratings yet
- SeizuresDocument3 pagesSeizuressarguss14No ratings yet
- Lecturer of Neurology Mansoura Faculty of Medicine: Ashraf El-Mitwalli, MDDocument122 pagesLecturer of Neurology Mansoura Faculty of Medicine: Ashraf El-Mitwalli, MDCarolina TulanNo ratings yet