You might also like
- Polycystic Ovarian Syndrome (PCOS) : ComplicationsDocument1 pagePolycystic Ovarian Syndrome (PCOS) : ComplicationsSahnia Uli SilitongaNo ratings yet
- 61 Microbiological Examination of Nonsterile Products - Microbial Enumeration Tests PDFDocument6 pages61 Microbiological Examination of Nonsterile Products - Microbial Enumeration Tests PDFStefania OsorioNo ratings yet
- Á61Ñ Microbiological Examination of Nonsterile Products: Microbial Enumeration TestsDocument7 pagesÁ61Ñ Microbiological Examination of Nonsterile Products: Microbial Enumeration TestsSpectre SpectreNo ratings yet
- Microbiologicos USPDocument7 pagesMicrobiologicos USPlazaro.oscar1117No ratings yet
- Á61Ñ Microbiological Examination of Nonsterile Products: Microbial Enumeration TestsDocument7 pagesÁ61Ñ Microbiological Examination of Nonsterile Products: Microbial Enumeration TestsjohncweslyNo ratings yet
- Characterization of Methicillin-Resistant Staphylococcus Aureus Isolated From Retail Raw Chicken Meat in JapanDocument4 pagesCharacterization of Methicillin-Resistant Staphylococcus Aureus Isolated From Retail Raw Chicken Meat in JapanIrham SupriajiNo ratings yet
- Usp-Nf 61 Microbiological Examination of Nonsterile Products Microbial Enumeration TestsDocument7 pagesUsp-Nf 61 Microbiological Examination of Nonsterile Products Microbial Enumeration TestsLuisa Hidalgo MeschiniNo ratings yet
- USP-NF 〈61〉 Microbiological Examination of Nonsterile Products - Microbial Enumeration TestsDocument7 pagesUSP-NF 〈61〉 Microbiological Examination of Nonsterile Products - Microbial Enumeration TestsDuy Tien NguyenNo ratings yet
- USP 43 Cap 61Document7 pagesUSP 43 Cap 61Laura BriceñoNo ratings yet
- ESBL SalmonellaDocument12 pagesESBL SalmonellaDaranee Nak-opatNo ratings yet
- Identification: of Gram-Negative Non-Fermenters and Oxidase-Positive Fermenters by The Oxi/Ferm TubeDocument8 pagesIdentification: of Gram-Negative Non-Fermenters and Oxidase-Positive Fermenters by The Oxi/Ferm TubeJack QuizonNo ratings yet
- 〈61〉 MICROBIOLOGICAL EXAMINATION OF NONSTERILE PRODUCTS MICROBIAL ENUMERATION TESTSDocument11 pages〈61〉 MICROBIOLOGICAL EXAMINATION OF NONSTERILE PRODUCTS MICROBIAL ENUMERATION TESTSviviNo ratings yet
- Implementsi PMK 8-2015 PPRADocument47 pagesImplementsi PMK 8-2015 PPRAMaya DamanikNo ratings yet
- Prof. Dr. Kuntaman, DR.,MS, SPMK (K)Document27 pagesProf. Dr. Kuntaman, DR.,MS, SPMK (K)navytiaraNo ratings yet
- Materi DrharrypDocument38 pagesMateri DrharrypAnnisa Aisyha MalikNo ratings yet
- Implementsi PMK 8-2015 PPRA (DR Joni) PDFDocument45 pagesImplementsi PMK 8-2015 PPRA (DR Joni) PDFAlfa MonicaNo ratings yet
- DR Mahesh PaperDocument3 pagesDR Mahesh PaperDrdariyaNo ratings yet
- In Vitro Investigation of The Antimicrobial Effect of Three Bisphosphonates Against Different Bacterial StrainsDocument8 pagesIn Vitro Investigation of The Antimicrobial Effect of Three Bisphosphonates Against Different Bacterial StrainsAmar ElezovicNo ratings yet
- Microbial EnumerationDocument7 pagesMicrobial Enumerationvivek pattaniNo ratings yet
- Subjects&Methods: Place of StudyDocument17 pagesSubjects&Methods: Place of StudyMahmoud OmNo ratings yet
- Manual of Diagnostic Antibodies For Immunohistology - 1841101001Document539 pagesManual of Diagnostic Antibodies For Immunohistology - 1841101001dudapaskasNo ratings yet
- 61 Microbial TestingDocument9 pages61 Microbial TestingManojNo ratings yet
- 1155 Ijsem003285Document7 pages1155 Ijsem0032850237Đặng Quốc CườngNo ratings yet
- Journal of Infection: Letter To The EditorDocument3 pagesJournal of Infection: Letter To The EditorRafika RaraNo ratings yet
- In Vitro Antifungal Susceptibilities of Cryptococcus Neoformans From Pigeon Droppings, Cats, and Human Sources in Bangkok, ThailandDocument2 pagesIn Vitro Antifungal Susceptibilities of Cryptococcus Neoformans From Pigeon Droppings, Cats, and Human Sources in Bangkok, ThailandPrasert ApiwatsiriNo ratings yet
- Evaluation of Six Commercial Products For Colistin Susceptibility Testing in EnterobacteralesDocument35 pagesEvaluation of Six Commercial Products For Colistin Susceptibility Testing in EnterobacteralessharvaniNo ratings yet
- Central Session FungalDocument17 pagesCentral Session Fungaldocjeevan89No ratings yet
- 1c - Interpretasi - Klinik - Mikro - PRADIK PPDS 2021Document35 pages1c - Interpretasi - Klinik - Mikro - PRADIK PPDS 2021Herbanu Haryo PramonoNo ratings yet
- BM 2.3 Murti AndriastutiDocument27 pagesBM 2.3 Murti AndriastutiAbdullah ShiddiqNo ratings yet
- Wa0023Document3 pagesWa0023Nishar AkhtarNo ratings yet
- Riemerella AntipestiferDocument4 pagesRiemerella Antipestifertopham69No ratings yet
- Httpresearch - Rmu.ac - Thrdi Misuploadfullreport1631092607.PDF 2Document97 pagesHttpresearch - Rmu.ac - Thrdi Misuploadfullreport1631092607.PDF 2Phonpawee KhodkiaoNo ratings yet
- Molecular Controls For Gastro-Intestinal Infection Testing - v2Document1 pageMolecular Controls For Gastro-Intestinal Infection Testing - v2moutasim mohammadNo ratings yet
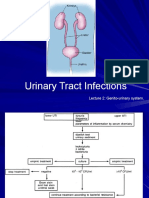
- Urinary Tract Infections: Lecture 2: Genito-Urinary SystemDocument44 pagesUrinary Tract Infections: Lecture 2: Genito-Urinary Systemangelica gloryNo ratings yet
- Gram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)Document2 pagesGram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)jen nalusNo ratings yet
- DR Irwanto's SlidesDocument22 pagesDR Irwanto's SlidesAstria PermanaNo ratings yet
- Current Technology For The Industrial Manufacture of Snake AntivenomsDocument59 pagesCurrent Technology For The Industrial Manufacture of Snake AntivenomsLizbeth OchoaNo ratings yet
- Tmp6a78 TMPDocument5 pagesTmp6a78 TMPFrontiersNo ratings yet
- 4-5-6.PATHOMECHANISM - ANGOL 2013aDocument178 pages4-5-6.PATHOMECHANISM - ANGOL 2013azahra eskandarianNo ratings yet
- PS5 3 (Japan)Document17 pagesPS5 3 (Japan)Reema IshaqNo ratings yet
- Ocular Antibiotics and Anti-Infectives: Regis P. Kowalski, MS, M (ASCP)Document16 pagesOcular Antibiotics and Anti-Infectives: Regis P. Kowalski, MS, M (ASCP)Maria SpatariNo ratings yet
- 10 1292@jvms 20-0017Document22 pages10 1292@jvms 20-0017Nadia AbarcaNo ratings yet
- 511 jmm000460Document6 pages511 jmm000460Nur LaylaNo ratings yet
- Program Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah SakitDocument34 pagesProgram Pengendalian Resistensi Antimikroba: (PPRA) Di Rumah Sakitevy sari sutrisnaningsih100% (1)
- Etiological Spectrum and Antimicrobial Resistance Among Bacterial Pathogen Association With Urinary Tract Infection in Wasit Governorate/ IraqDocument11 pagesEtiological Spectrum and Antimicrobial Resistance Among Bacterial Pathogen Association With Urinary Tract Infection in Wasit Governorate/ IraqCentral Asian StudiesNo ratings yet
- Analysis of Antibiotic Residues: Ridascreen®/EuroproximaDocument3 pagesAnalysis of Antibiotic Residues: Ridascreen®/EuroproximaSyeda Nazish BokhariNo ratings yet
- Research Article Staphylococcus AureusDocument7 pagesResearch Article Staphylococcus Aureussarim AzizNo ratings yet
- 1 Recently Approved AntibioticsDocument29 pages1 Recently Approved Antibioticslpa.ufmt.enfNo ratings yet
- 突變檢測系統Document83 pages突變檢測系統coffee910603No ratings yet
- Kingella SpeciesDocument23 pagesKingella Specieslongphan0619No ratings yet
- Student, Faculty of Veterinary Medicine, University of Nairobi P.O. Box 29053, 00625, KangemiDocument8 pagesStudent, Faculty of Veterinary Medicine, University of Nairobi P.O. Box 29053, 00625, Kangemidominic KingoriNo ratings yet
- 1 s2.0 S1075996421001311 MainDocument5 pages1 s2.0 S1075996421001311 MainMaryHope OluwatosinNo ratings yet
- Protocolo Acelerado Desde HemocultivoDocument4 pagesProtocolo Acelerado Desde HemocultivoSharom Zelene Cordova RomanNo ratings yet
- 7.1b - ABgram - KARS - JKT - 2017 (Prof Kuntaman)Document23 pages7.1b - ABgram - KARS - JKT - 2017 (Prof Kuntaman)MeylinNo ratings yet
- MDR Pathogens in ICU: Azit Kumar PulagurthaDocument37 pagesMDR Pathogens in ICU: Azit Kumar PulagurthaAjitkumar PulagurthaNo ratings yet
- M51S1Document2 pagesM51S1Hassab SaeedNo ratings yet
- 16.kuntaman Bacteri Specimen SKTDocument26 pages16.kuntaman Bacteri Specimen SKTHesty NoviantieNo ratings yet
- Aac 00642-17Document8 pagesAac 00642-17Robert StryjakNo ratings yet
- Instructive Wound Dressings Silk Fibroin and Paramylon RevolutionFrom EverandInstructive Wound Dressings Silk Fibroin and Paramylon RevolutionNo ratings yet
- Molecular Breeding and Genetics of Applied MicroorganismsFrom EverandMolecular Breeding and Genetics of Applied MicroorganismsKenji SakaguchiNo ratings yet
- Small Molecular Immunomodifiers of Microbial Origin: Fundamental and Clinical Studies of BestatinFrom EverandSmall Molecular Immunomodifiers of Microbial Origin: Fundamental and Clinical Studies of BestatinHamao UmezawaNo ratings yet
- Pharmaceutical Nanotechnology Novel Nanoemulsion High EnergyDocument22 pagesPharmaceutical Nanotechnology Novel Nanoemulsion High EnergyMitesh ChauhanNo ratings yet
- Lec - 9 Concept of Angiogenesis and Importance of Nutraceuticals in Health PromotionDocument18 pagesLec - 9 Concept of Angiogenesis and Importance of Nutraceuticals in Health PromotionDivya DiyaNo ratings yet
- Week 9 - Drug (Control) Ordinance 1982Document10 pagesWeek 9 - Drug (Control) Ordinance 1982Runa akterNo ratings yet
- Vit CDocument10 pagesVit C3/2 no.34 สรัญญากร สีหาราชNo ratings yet
- GOKU-Rheumatology-SLE-OTHER-Connective Tissue Diseases and VasculitisDocument30 pagesGOKU-Rheumatology-SLE-OTHER-Connective Tissue Diseases and VasculitisCas BuNo ratings yet
- Quickstart+Guide+to+Microdosing+Ayahuasca+v2 1Document20 pagesQuickstart+Guide+to+Microdosing+Ayahuasca+v2 1Víctor Lucia SánchezNo ratings yet
- Sleep DisordersDocument32 pagesSleep DisordersSana Sheikh KashifNo ratings yet
- Rusan Pharma Product ListDocument4 pagesRusan Pharma Product ListSanjay SharmaNo ratings yet
- Substance AbuseDocument16 pagesSubstance AbuseAkansha JohnNo ratings yet
- Allantoin Soothing EffectDocument17 pagesAllantoin Soothing EffectValentina CarreroNo ratings yet
- Teaching Plan - Theory PCDocument8 pagesTeaching Plan - Theory PCHarshada mahajanNo ratings yet
- Ethanol Intoxication in Adults - UpToDateDocument16 pagesEthanol Intoxication in Adults - UpToDateBogdanBudusanNo ratings yet
- Antifungal Properties of BreadfruitDocument16 pagesAntifungal Properties of BreadfruitEllen PortezNo ratings yet
- Order InformationDocument5 pagesOrder InformationKattaleyaNo ratings yet
- Carvalho Et Al, 2014 - Regulation of Herbal Medicines in BrazilDocument4 pagesCarvalho Et Al, 2014 - Regulation of Herbal Medicines in BrazilLu JunqueiraNo ratings yet
- B Pharm 6 Sem Pharmalite - inDocument18 pagesB Pharm 6 Sem Pharmalite - insatyaroxx258No ratings yet
- DaftarobatDocument23 pagesDaftarobatJuon Vairzya AnggraeniNo ratings yet
- Recent Progress in Transglutaminase-Mediated Assembly of Antibody-Drug ConjugatesDocument13 pagesRecent Progress in Transglutaminase-Mediated Assembly of Antibody-Drug ConjugatesRosita HandayaniNo ratings yet
- Medication AssignmentDocument5 pagesMedication Assignmentapi-525323558No ratings yet
- GI Bleed InpatientDocument17 pagesGI Bleed InpatientAnisaNo ratings yet
- Introduction To Regulatory AffairsDocument15 pagesIntroduction To Regulatory AffairsCyclone Pharmaceuticals Pvt Ltd PuneNo ratings yet
- Liposomal IronDocument6 pagesLiposomal IronPiyush KhetrapalNo ratings yet
- Project Chapters MayowaDocument49 pagesProject Chapters Mayowanjoku danielNo ratings yet
- Benefits and Risks To Biosimilars: From A Patient Perspective?Document15 pagesBenefits and Risks To Biosimilars: From A Patient Perspective?drtanoyboseNo ratings yet
- Pharmacokinetics in Obese Patients: Luc Ec de Baerdemaeker MD Eric P Mortier MD DSC Michel MRF Struys MD PHDDocument4 pagesPharmacokinetics in Obese Patients: Luc Ec de Baerdemaeker MD Eric P Mortier MD DSC Michel MRF Struys MD PHDMahmood RahmanNo ratings yet
- Complications of Fractional CO2 Laser Resurfacing 2009Document6 pagesComplications of Fractional CO2 Laser Resurfacing 2009irwan junNo ratings yet
- NsaidDocument17 pagesNsaidnoviasinataNo ratings yet
- LohiaDocument11 pagesLohiastanleyNo ratings yet
- Indometacin - Grupa 4Document5 pagesIndometacin - Grupa 4Daniela PopaNo ratings yet