You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Suraj Gupte - Differential Diagnosis in PEDIATRICS - 40 Including Color Atl PDFDocument619 pagesSuraj Gupte - Differential Diagnosis in PEDIATRICS - 40 Including Color Atl PDFRichard MelialaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Project Proposal: By: Ian Carl Esgra Frenzy Felamin Cyril John Tan Kenneth PadillaDocument14 pagesProject Proposal: By: Ian Carl Esgra Frenzy Felamin Cyril John Tan Kenneth PadillaKENNETH PADILLA100% (2)
- DIAGNOSIS Hyperthermia Related To Increased Metabolic Rate, Illness. ASSESSMENT SubjectiveDocument1 pageDIAGNOSIS Hyperthermia Related To Increased Metabolic Rate, Illness. ASSESSMENT Subjectivemawel100% (1)
- The Global Pharmaceutical Industry Case Study Scenario PlanningDocument4 pagesThe Global Pharmaceutical Industry Case Study Scenario PlanningIke Ten100% (1)
- JCDR 11 SC09Document4 pagesJCDR 11 SC09hollNo ratings yet
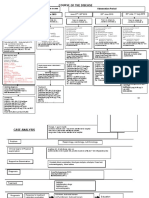
- Course of The Disease: Observation Period 25 June 2019 26 June 2019 Admission Adopted As A CaseDocument2 pagesCourse of The Disease: Observation Period 25 June 2019 26 June 2019 Admission Adopted As A CasehollNo ratings yet
- Custard PuddingDocument1 pageCustard PuddinghollNo ratings yet
- 10 5772@54652 PDFDocument32 pages10 5772@54652 PDFhollNo ratings yet
- Clinical Guidelines For The Use of Parenteral and Enteral Nutrition in Adult and Pediatric Patients, 2009Document5 pagesClinical Guidelines For The Use of Parenteral and Enteral Nutrition in Adult and Pediatric Patients, 2009hollNo ratings yet
- Hubungan Antara Kadar Asam Urat Dengan Tekanan Darah Pada Anak Obes Di Kecamatan Talawaan Kabupaten Minahasa UtaraDocument7 pagesHubungan Antara Kadar Asam Urat Dengan Tekanan Darah Pada Anak Obes Di Kecamatan Talawaan Kabupaten Minahasa UtarahollNo ratings yet
- 09 Ra Expnded Dengue PDFDocument5 pages09 Ra Expnded Dengue PDFhollNo ratings yet
- Alcohol Abstinence in Drinkers With Atrial FibrillationDocument16 pagesAlcohol Abstinence in Drinkers With Atrial FibrillationDaniela PopNo ratings yet
- Equine Science 4th Edition Ebook PDFDocument61 pagesEquine Science 4th Edition Ebook PDFjoshua.little480100% (42)
- Elective ReportDocument3 pagesElective ReportBanu ThuraisingamNo ratings yet
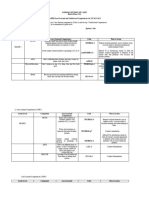
- Nursing Department: Assessment Explanation of The Problem Objective Interventions Rationale EvaluationDocument2 pagesNursing Department: Assessment Explanation of The Problem Objective Interventions Rationale EvaluationNelly CruzNo ratings yet
- Iep Manatee PKTDocument12 pagesIep Manatee PKTapi-284370848No ratings yet
- Research ProjectDocument45 pagesResearch ProjectTeam MatrixNo ratings yet
- Digitalization in Nursing ServicesDocument4 pagesDigitalization in Nursing ServicesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vioxx and The Merck Team Effort: Institutions in CrisisDocument22 pagesVioxx and The Merck Team Effort: Institutions in CrisisRebecca LiuNo ratings yet
- Sistem Reproduksi Wanita-Uswatun Hasanah 195037Document13 pagesSistem Reproduksi Wanita-Uswatun Hasanah 195037Uswatun HasanahNo ratings yet
- The McKenzie Method For Low Back PainDocument9 pagesThe McKenzie Method For Low Back PainRupesh Mamidi100% (1)
- The Ebn A. Evidence Based Nursing For Level III General QuestionDocument7 pagesThe Ebn A. Evidence Based Nursing For Level III General QuestionAvyNo ratings yet
- The Medical TranscriptionistDocument22 pagesThe Medical TranscriptionistrimeoznekNo ratings yet
- HypnosisDocument11 pagesHypnosisirish x100% (1)
- Baby Bloom BrochureDocument4 pagesBaby Bloom BrochureDewi LarasatiNo ratings yet
- Death Investigation: Death - Organ Donation Act of 1991 Investigation of DeathDocument5 pagesDeath Investigation: Death - Organ Donation Act of 1991 Investigation of DeathClaude PosadasNo ratings yet
- FINAL YEAR ReportDocument25 pagesFINAL YEAR Report4AL20AI026 NIKHIL G BNo ratings yet
- Curriculum Vitae DR Andrea GilkisonDocument5 pagesCurriculum Vitae DR Andrea GilkisonysNo ratings yet
- PositrimDocument51 pagesPositrimapi-19978941No ratings yet
- Least Learned Skills in MapehDocument6 pagesLeast Learned Skills in MapehDiana ValienteNo ratings yet
- Prometric Questions: Reviewed By:dr - Mohamed Soliman Call: +201016640110Document215 pagesPrometric Questions: Reviewed By:dr - Mohamed Soliman Call: +201016640110Mallu StreamerNo ratings yet
- Statement From Health Canada and The Public Health Agency of Canada On Aug. 11, 2021Document1 pageStatement From Health Canada and The Public Health Agency of Canada On Aug. 11, 2021Toronto StarNo ratings yet
- Care ReportDocument23 pagesCare ReportSindi Muthiah UtamiNo ratings yet
- Safety Data Sheet: Effective Date 06.09.2010Document8 pagesSafety Data Sheet: Effective Date 06.09.2010Vevi Elvira SiicewetvirapoenyanyasiiEapNo ratings yet
- Lumbar Radiculopathy 5 18Document2 pagesLumbar Radiculopathy 5 18Youzuf IqbalNo ratings yet
- Analisis Penyebab Insiden Pasien Jatuh Di Rawat Inap Rs. Y Di Kota PadangDocument9 pagesAnalisis Penyebab Insiden Pasien Jatuh Di Rawat Inap Rs. Y Di Kota Padangjangmed rsghNo ratings yet