You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Faculty: Department: Sub: Topic: Lecturer Class: PresentaterDocument13 pagesFaculty: Department: Sub: Topic: Lecturer Class: PresentaterCabdiladif Ahmed McrfNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- 15.ectopic Pregnancy 15Document15 pages15.ectopic Pregnancy 15Cabdiladif Ahmed McrfNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Drugs Used in AneasthesiaDocument73 pagesDrugs Used in AneasthesiaCabdiladif Ahmed McrfNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Disorders of Potassium: Dr. YabarowDocument43 pagesDisorders of Potassium: Dr. YabarowCabdiladif Ahmed McrfNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Psychosis-SchizophreniaDocument14 pagesPsychosis-SchizophreniaCabdiladif Ahmed McrfNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- PigmentationDocument28 pagesPigmentationCabdiladif Ahmed McrfNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Shock: Dr. Fartun Orey MBCHB, Mmed PaedDocument16 pagesShock: Dr. Fartun Orey MBCHB, Mmed PaedCabdiladif Ahmed McrfNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Opioids: Zainab Sabrie Pharmd MpharmDocument32 pagesOpioids: Zainab Sabrie Pharmd MpharmCabdiladif Ahmed McrfNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Birth Asphyxia and HIE: Dr. Fartun OreyDocument9 pagesBirth Asphyxia and HIE: Dr. Fartun OreyCabdiladif Ahmed McrfNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Dr. Fartun Orey MBCHB, Mmed PaedDocument14 pagesDr. Fartun Orey MBCHB, Mmed PaedCabdiladif Ahmed McrfNo ratings yet
- Back PainDocument18 pagesBack PainCabdiladif Ahmed McrfNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
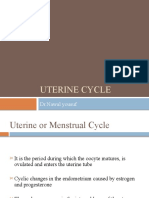
- Uterine CyclesDocument15 pagesUterine CyclesCabdiladif Ahmed McrfNo ratings yet
- Implantation & Second WeekDocument18 pagesImplantation & Second WeekCabdiladif Ahmed McrfNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- General EmbryologyDocument19 pagesGeneral EmbryologyCabdiladif Ahmed McrfNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Brown-Sequard Syndrome From Cervical Disc Herniation, A Case Report and Review of LiteratureDocument3 pagesBrown-Sequard Syndrome From Cervical Disc Herniation, A Case Report and Review of LiteratureCabdiladif Ahmed McrfNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Developing An Implementation Research Proposal Print VersionDocument68 pagesDeveloping An Implementation Research Proposal Print VersionndistantiNo ratings yet
- Sample Doctors Note For StudentDocument1 pageSample Doctors Note For StudentWaldo SchobbenNo ratings yet
- Podoconiosis: What Is It and What Can We Do About It?Document7 pagesPodoconiosis: What Is It and What Can We Do About It?yoga yogafenkanoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- YerseniosisDocument7 pagesYerseniosissomebody_maNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Infectious Hazards of Dead BodiesDocument3 pagesThe Infectious Hazards of Dead Bodiespenn hicksNo ratings yet
- Communicable Disease NursingDocument41 pagesCommunicable Disease NursingPagarigan VianNo ratings yet
- Issues - Cultural & EnvironmentalDocument29 pagesIssues - Cultural & EnvironmentalFatima GilbuenaNo ratings yet
- Impact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyDocument6 pagesImpact of Type 1 Versus Type 2 Diabetes On Developing Herpes Zoster and Post-Herpetic Neuralgia: A Population-Based Cohort StudyStella SulartoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Iraqi Injury Surveillance System Annual Report 2013Document46 pagesIraqi Injury Surveillance System Annual Report 2013bejarhasanNo ratings yet
- Pathology of The RetinaDocument19 pagesPathology of The RetinaAlex OlahNo ratings yet
- Laboratory Test Report: Test Name Result Sars-Cov-2Document1 pageLaboratory Test Report: Test Name Result Sars-Cov-2Karthikeya MoorthyNo ratings yet
- Coronary Heart Disease The Framingham Study: MannDocument21 pagesCoronary Heart Disease The Framingham Study: MannYunlong LiuNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Hypertension JDHHDDDocument5 pagesHypertension JDHHDDabcxyz15021999No ratings yet
- CHALHOUB, Sidney (1993) The Politics of Disease Control. Yellow Fever and Race in Nineteenth Century Rio de JaneiroDocument24 pagesCHALHOUB, Sidney (1993) The Politics of Disease Control. Yellow Fever and Race in Nineteenth Century Rio de JaneiroDiogo CãoNo ratings yet
- Heart Failure Clinical Records DatasetDocument6 pagesHeart Failure Clinical Records DatasetOcta HutapeaNo ratings yet
- MG PosterDocument1 pageMG PosterNataShini RajaRatnamNo ratings yet
- 10 Penyakit Terbesar BPJSDocument6 pages10 Penyakit Terbesar BPJSWeni ArdiantiNo ratings yet
- New Research Posters: ResultsDocument1 pageNew Research Posters: ResultsKristoffer LoquiasNo ratings yet
- Brain InfectionDocument8 pagesBrain Infectionsistla naveenNo ratings yet
- Swot Analysis Health Strength BP Is Normal Fbs or Fasting Blood Sugar Is 4.21 Urinalysis Is 0-1 No Infection Healthy Bones Physically Fit WeaknessesDocument1 pageSwot Analysis Health Strength BP Is Normal Fbs or Fasting Blood Sugar Is 4.21 Urinalysis Is 0-1 No Infection Healthy Bones Physically Fit WeaknessesJymaer GeromoNo ratings yet
- Bernardino Ramazzini (1633-1714)Document2 pagesBernardino Ramazzini (1633-1714)uknandiNo ratings yet
- Introduction To EpidemiologyDocument9 pagesIntroduction To EpidemiologyJhon Albert RobledoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Septic Shock: Stephen Trzeciak, R. Phillip Dellinger, and Joseph E. ParrilloDocument14 pagesSeptic Shock: Stephen Trzeciak, R. Phillip Dellinger, and Joseph E. ParrilloMedranoReyesLuisinNo ratings yet
- March 11-12, 2023 Camp Maria Aurora Panicuason, Naga CityDocument3 pagesMarch 11-12, 2023 Camp Maria Aurora Panicuason, Naga CityAmika G. NantizaNo ratings yet
- Health Fitness Certificate For The Purposes of Permission To Work in Confined SpaceDocument6 pagesHealth Fitness Certificate For The Purposes of Permission To Work in Confined SpaceNur ShaNo ratings yet
- RACMA Approved Masters Programs - 2020Document1 pageRACMA Approved Masters Programs - 2020Crystal ZawNo ratings yet
- Industry Corporate & Business Effects On PerformanceDocument19 pagesIndustry Corporate & Business Effects On PerformanceRenold FernandesNo ratings yet
- Posterior Uveitis HandoutDocument4 pagesPosterior Uveitis Handoutdanny wiryaNo ratings yet
- DR Kamlesh Verma - OncologistDocument10 pagesDR Kamlesh Verma - OncologistDr Kamlesh VermaNo ratings yet
- Clerk Sheet Imed and ObsDocument4 pagesClerk Sheet Imed and ObsGrace PhiriNo ratings yet