You might also like
- Alex Schiffer - Joe Cell - Experimenters Guide To The Joe CellDocument130 pagesAlex Schiffer - Joe Cell - Experimenters Guide To The Joe CellAnonymous UwXe23xNo ratings yet
- How To Pick Up Bitches.A5Document26 pagesHow To Pick Up Bitches.A5Tobias BlassNo ratings yet
- Assignment 4Document8 pagesAssignment 4api-328441669100% (1)
- Matthew Williams Charging DocsDocument3 pagesMatthew Williams Charging DocsCurtis CartierNo ratings yet
- Anatomy and Physiology of ZombiesDocument12 pagesAnatomy and Physiology of ZombiesdsolisNo ratings yet
- Cushing's SyndromeDocument21 pagesCushing's Syndromeadamu mohammadNo ratings yet
- Cushing's SyndromeDocument6 pagesCushing's SyndromeAtiqahNo ratings yet
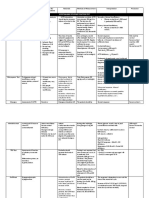
- Indications Possible SE/ Contraindications Rationale Methods of Measurement Interpretation PrecautionDocument5 pagesIndications Possible SE/ Contraindications Rationale Methods of Measurement Interpretation PrecautionJohn Christopher LucesNo ratings yet
- PBL 12 - Adrenal GlandsDocument7 pagesPBL 12 - Adrenal GlandsKrishna OochitNo ratings yet
- Cushing DiseaseDocument24 pagesCushing DiseaseSuci AlimaNo ratings yet
- 4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosDocument19 pages4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosBitz Basos ViadoNo ratings yet
- Cushing's Decision App - Glossary of Terms 2Document3 pagesCushing's Decision App - Glossary of Terms 2Erhan ErtuçNo ratings yet
- Adrenal DisordersDocument72 pagesAdrenal DisordersMinilik DersehNo ratings yet
- Lectur 09 Measurement of MetabolitesDocument38 pagesLectur 09 Measurement of MetabolitesNavoda ThathsaraniNo ratings yet
- Diseases of Adrenal Gland: DR Samir ChakrabortyDocument14 pagesDiseases of Adrenal Gland: DR Samir ChakrabortyJaymalyaNo ratings yet
- Adrenal DiseasesDocument66 pagesAdrenal DiseasesNebiyu NegaNo ratings yet
- Adrenal DisorderDocument19 pagesAdrenal DisorderYemata HailuNo ratings yet
- Endocrine Physiolgy - Lec 04 - Intake 40 - Adrenal GlandDocument30 pagesEndocrine Physiolgy - Lec 04 - Intake 40 - Adrenal Glanddidulalakshitha39No ratings yet
- Review of Laboratory and Diagnostic TestsDocument41 pagesReview of Laboratory and Diagnostic TestsPutri Anggraini Rusanti100% (1)
- Adrenal GlandDocument75 pagesAdrenal GlandPamela MendozaNo ratings yet
- Review of LaboratoryDocument48 pagesReview of LaboratoryIkhar RidhoNo ratings yet
- Endocrine PBL Trigger 3Document6 pagesEndocrine PBL Trigger 3Ho Yong WaiNo ratings yet
- Cushing Syndrome: M.Sc. (N) 1 YearDocument30 pagesCushing Syndrome: M.Sc. (N) 1 YearRanjana SharmaNo ratings yet
- Diseases of The Adrenal GlandsDocument27 pagesDiseases of The Adrenal GlandsPurnima ChoudhuryNo ratings yet
- المحاطرة الاولة كيمياء سريريةDocument35 pagesالمحاطرة الاولة كيمياء سريريةMohamedErrmaliNo ratings yet
- Excretion (Dr. Imran Ashraf)Document44 pagesExcretion (Dr. Imran Ashraf)Abdul WahabNo ratings yet
- Adrenal Function: Adrenocorticotropic HormoneDocument11 pagesAdrenal Function: Adrenocorticotropic HormonehansenNo ratings yet
- Principles and Application of Investigative and Imaging TechniquesDocument54 pagesPrinciples and Application of Investigative and Imaging TechniquesLal NandaniNo ratings yet
- Endocrine N41Document3 pagesEndocrine N41ashafernandesssNo ratings yet
- Congenital Adrenal HyperplasiaDocument15 pagesCongenital Adrenal Hyperplasiaokwadha simionNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- 7 Elimination StudentDocument42 pages7 Elimination StudentSelena MoonNo ratings yet
- Cardiac DiagnosticsDocument97 pagesCardiac DiagnosticsNaomi Anne Asunto100% (1)
- The Adrenal GlandDocument39 pagesThe Adrenal GlandSteph VistalNo ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- Adrenal Gland - DR CokerDocument59 pagesAdrenal Gland - DR CokerIshaqNo ratings yet
- Endocrine Disorders NotesDocument14 pagesEndocrine Disorders NotesSarahMelissaNo ratings yet
- 5) Adrenal GlandDocument74 pages5) Adrenal GlandABUBEKER BESHIRNo ratings yet
- Adrenal Hormone 2018 PDFDocument66 pagesAdrenal Hormone 2018 PDFrosyidafiaNo ratings yet
- Hypercortisolism (Cushing' S Syndrome)Document30 pagesHypercortisolism (Cushing' S Syndrome)Denis R. D. SatriaNo ratings yet
- Hormon AdrenalDocument76 pagesHormon AdrenalgitafazaNo ratings yet
- Adrenal GlandDocument32 pagesAdrenal GlandAlok KumarNo ratings yet
- The Hypothalamo-Pituitary-Adrenocortical Axis: Dr. Noelle Orata Mount Kenya UniversityDocument49 pagesThe Hypothalamo-Pituitary-Adrenocortical Axis: Dr. Noelle Orata Mount Kenya UniversityvivianNo ratings yet
- 07 PhysiologyDocument238 pages07 PhysiologyMahmoud AbuAwadNo ratings yet
- Dexamethasone Suppression TestDocument3 pagesDexamethasone Suppression TestMelisa MalikNo ratings yet
- Clinical Chemistry: Pmls - 1Document36 pagesClinical Chemistry: Pmls - 1ICE ADRIENNE OCAMPONo ratings yet
- 10 The Adrenal Gland Aldosterone2017 1Document27 pages10 The Adrenal Gland Aldosterone2017 1Tariq Jamil KoraiNo ratings yet
- Pharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDocument24 pagesPharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDebasish SanyalNo ratings yet
- Grand Round Case Presentation: by DR Sanjay Khare MD MedicineDocument19 pagesGrand Round Case Presentation: by DR Sanjay Khare MD MedicineHrishikeshNo ratings yet
- ENDO 22 SCL Data Interpretation of Adrenocortical DysfunctionDocument41 pagesENDO 22 SCL Data Interpretation of Adrenocortical DysfunctionNazreen sofia HazleenNo ratings yet
- 10 The Adrenal Gland Aldosterone2017 1Document27 pages10 The Adrenal Gland Aldosterone2017 1Hassan AhmedNo ratings yet
- Adrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaDocument34 pagesAdrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaMahmoud Abu MayalehNo ratings yet
- Pathophysilogy of Cushing Dse by OsmosisDocument4 pagesPathophysilogy of Cushing Dse by OsmosisEdrea MendezNo ratings yet
- Master The Wards - Internal Medicine - 1Document16 pagesMaster The Wards - Internal Medicine - 1rayousufNo ratings yet
- Acute Adrenal CrisisDocument27 pagesAcute Adrenal CrisisHemanthNo ratings yet
- Endoc, Pancreas, ThyroidDocument9 pagesEndoc, Pancreas, ThyroidKatrina Vianca DecapiaNo ratings yet
- Week 7. COURSE TASK - Case Study - Cushing SyndromeDocument5 pagesWeek 7. COURSE TASK - Case Study - Cushing SyndromeTerence SalamatNo ratings yet
- Hiperosmolar Non KetotikDocument24 pagesHiperosmolar Non KetotikMunawwar AweNo ratings yet
- Clinical Chemistry Lec 5Document70 pagesClinical Chemistry Lec 5salamshakir56No ratings yet
- 208-Cushing's Syndrome PDFDocument13 pages208-Cushing's Syndrome PDFJannat JabbarNo ratings yet
- Adrenal DiseaseDocument77 pagesAdrenal DiseaseNzau Muange100% (1)
- Adrenal GlandDocument46 pagesAdrenal GlandhSANNo ratings yet
- Addison's DiseaseDocument57 pagesAddison's DiseaseVie Delvia100% (4)
- Acute Viral Hepatitis: Jonathan WalaDocument49 pagesAcute Viral Hepatitis: Jonathan WalaAntony WaithakaNo ratings yet
- Chronic Interstitial (Restrictive Infiltrative) Lung DiseasesDocument44 pagesChronic Interstitial (Restrictive Infiltrative) Lung DiseasesAntony WaithakaNo ratings yet
- Respiratory System: Dr. Noelle Orata Kenyatta University MBCHB IiiDocument23 pagesRespiratory System: Dr. Noelle Orata Kenyatta University MBCHB IiiAntony WaithakaNo ratings yet
- Lesson 1: Chemical Pathology of The Pituitary and Hypothalamus Lesson Learning OutcomesDocument3 pagesLesson 1: Chemical Pathology of The Pituitary and Hypothalamus Lesson Learning OutcomesAntony WaithakaNo ratings yet
- Lesson 2: Chemical Pathology of The ThyroidDocument2 pagesLesson 2: Chemical Pathology of The ThyroidAntony WaithakaNo ratings yet
- Lab Report 2Document13 pagesLab Report 2Unique GuyNo ratings yet
- What Muslim Invaders Really Did To IndiaDocument4 pagesWhat Muslim Invaders Really Did To IndiaTarek Fatah75% (16)
- PWC Orgdna The Key To Unlocking Your Companys PotentialDocument1 pagePWC Orgdna The Key To Unlocking Your Companys PotentialMinh Nguyễn TrọngNo ratings yet
- Ifa Tourneeausstellungen 2021 ENDocument112 pagesIfa Tourneeausstellungen 2021 ENsextoNo ratings yet
- Fomrhi 060Document40 pagesFomrhi 060rodolfoNo ratings yet
- ESUR Guidelines 10.0 Final VersionDocument46 pagesESUR Guidelines 10.0 Final Versionkon shireNo ratings yet
- The Role of Significance Tests1: D. R. CoxDocument22 pagesThe Role of Significance Tests1: D. R. CoxMusiur Raza AbidiNo ratings yet
- Zoom G2.1u English ManualDocument25 pagesZoom G2.1u English ManualKevin KerberNo ratings yet
- How To Judge DiseasesDocument2 pagesHow To Judge Diseasesmaharajkumar100% (1)
- SOC 1502 Learning Journal Unit 4Document29 pagesSOC 1502 Learning Journal Unit 4MangalisoNo ratings yet
- Da Drought 3 SongbookDocument99 pagesDa Drought 3 Songbookalex647No ratings yet
- Unit 4: For A Better Community Skills: Reading Why Do People Volunteer?Document5 pagesUnit 4: For A Better Community Skills: Reading Why Do People Volunteer?Hồng Duyên QuáchNo ratings yet
- World History Midterm Study GuideDocument2 pagesWorld History Midterm Study GuideMark JacksonNo ratings yet
- Incentives and BenefitsDocument58 pagesIncentives and Benefitskamaljit kaushikNo ratings yet
- Principles of Accounting - Course SyllabusDocument7 pagesPrinciples of Accounting - Course SyllabusChristian Emil ReyesNo ratings yet
- Caribbean Studies IADocument18 pagesCaribbean Studies IAansa_france100% (1)
- B.E. Mechanical Engineering: Affiliated Institutions Anna University of Technology ChennaiDocument17 pagesB.E. Mechanical Engineering: Affiliated Institutions Anna University of Technology Chennaivit_mechNo ratings yet
- Session 5 E4 - Ms. CabanillasDocument8 pagesSession 5 E4 - Ms. CabanillasLUIS MIGUEL LIMO PRIETONo ratings yet
- Job or BusinessDocument1 pageJob or Businessabhisek1987No ratings yet
- Design Approaches and Tools in Education and TrainingDocument296 pagesDesign Approaches and Tools in Education and Trainingmutia febri mouliNo ratings yet
- Prayer Before Study: Saint Joseph College, Maasin, Leyte Maasin City, Southern Leyte College of Teacher EducationDocument3 pagesPrayer Before Study: Saint Joseph College, Maasin, Leyte Maasin City, Southern Leyte College of Teacher EducationVencint LaranNo ratings yet
- PROM-12395-002 1114007 BRO QIAstat-Dx 0518 SPREAD WWDocument3 pagesPROM-12395-002 1114007 BRO QIAstat-Dx 0518 SPREAD WWTaty ElejaldeNo ratings yet
- People v. Panlilio, G.R. Nos. 113519-20 Case Digest (Criminal Procedure)Document4 pagesPeople v. Panlilio, G.R. Nos. 113519-20 Case Digest (Criminal Procedure)AizaFerrerEbina50% (2)
- Characteristics of Charismatic LeadershipDocument3 pagesCharacteristics of Charismatic LeadershipMuhammad Hashim Memon100% (1)
- Analysis and Interpretation of Assessment ResultsDocument84 pagesAnalysis and Interpretation of Assessment ResultsAlyanna Clarisse Padilla CamposNo ratings yet
- Concept-Paper-LP FINALDocument18 pagesConcept-Paper-LP FINALJodelyn Mae Singco CangrejoNo ratings yet