You might also like
- Childhood Pneumonia Diagnosis and TreatmentDocument65 pagesChildhood Pneumonia Diagnosis and TreatmentYemata HailuNo ratings yet
- 1 Urtd+eviDocument76 pages1 Urtd+eviIfabiyi OlaniyiNo ratings yet
- 2 Respiratory-InfectionsDocument61 pages2 Respiratory-InfectionsLana AiharaNo ratings yet
- Pneumonia Pathophysiology, Diagnosis and TreatmentDocument57 pagesPneumonia Pathophysiology, Diagnosis and TreatmentAnas FikriNo ratings yet
- 2 Respiratory-InfectionsDocument41 pages2 Respiratory-InfectionsYesi SaputriNo ratings yet
- Bronchitis LectureDocument46 pagesBronchitis LecturesanathanadharmaNo ratings yet
- Content 2Document16 pagesContent 2Prashant BhardwajNo ratings yet
- Pneumonia: Prof. Ezekiel M. WafulaDocument20 pagesPneumonia: Prof. Ezekiel M. Wafulaokwadha simion100% (1)
- Pneumonia & Lung AbscessDocument61 pagesPneumonia & Lung AbscessnewtypeNo ratings yet
- TherapyDocument100 pagesTherapyomolola adeogunNo ratings yet
- PneumoniaDocument5 pagesPneumoniasamtaynbNo ratings yet
- Syndrom of Consolidated Pulmonary Tissue. Pneumonia. Athelectasis. Andrei IchimDocument114 pagesSyndrom of Consolidated Pulmonary Tissue. Pneumonia. Athelectasis. Andrei IchimYan Sheng Ho100% (1)
- Community Acquired Pneumonia Nelson 400Document37 pagesCommunity Acquired Pneumonia Nelson 400fatima chrystelle nuñalNo ratings yet
- Aquire Pathology of Respiratory SystemDocument96 pagesAquire Pathology of Respiratory SystemBasit HussainNo ratings yet
- Unit X URTIDocument37 pagesUnit X URTIdiadiaidaNo ratings yet
- Pcap Didactics ChanDocument61 pagesPcap Didactics ChanValerie Anne BebitaNo ratings yet
- Prim Eng 2015-2016Document84 pagesPrim Eng 2015-2016humanNo ratings yet
- Wae'l Hayajneh: PneumoniaDocument14 pagesWae'l Hayajneh: PneumoniaRashed ShatnawiNo ratings yet
- Infectious Diseases-Dr - Mohammad Suliman - 15102010Document2 pagesInfectious Diseases-Dr - Mohammad Suliman - 15102010jordanmedicsNo ratings yet
- Diseases of the Lungs: Pneumonia, Bronchitis, AsthmaDocument72 pagesDiseases of the Lungs: Pneumonia, Bronchitis, AsthmaEdi Kerina SembiringNo ratings yet
- Pneumonii PedDocument19 pagesPneumonii PedVeronica NefiruNo ratings yet
- Week 1 TropMedDocument96 pagesWeek 1 TropMedmyqurandiaryNo ratings yet
- Respiratory Diseases Symptoms Causes TreatmentsDocument11 pagesRespiratory Diseases Symptoms Causes TreatmentsMichael Angelo SeñaNo ratings yet
- Respiratory System DisordersDocument9 pagesRespiratory System Disordersasop06No ratings yet
- PHAR 233-Pathophysiology of Respiratory System DiseasesDocument74 pagesPHAR 233-Pathophysiology of Respiratory System DiseasesLina RamojNo ratings yet
- PneumoniaDocument79 pagesPneumoniaEjiro OnoroNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument30 pagesMicrobial Diseases of The Respiratory SystemChristopher Eria Santiañez0% (1)
- Scarlet Fever: Caused by Group A StreptococciDocument24 pagesScarlet Fever: Caused by Group A StreptococciThomas GealonNo ratings yet
- _MICROMIDTERMSLABDocument27 pages_MICROMIDTERMSLABmicaellaabedejosNo ratings yet
- Antibiotics Training ManualDocument149 pagesAntibiotics Training ManualImran MullaNo ratings yet
- Bacterial Atypical (Interstitial) PneumoniaDocument24 pagesBacterial Atypical (Interstitial) Pneumoniamailkammar967No ratings yet
- Lower Respiratory Tract Infections: Bronchitis, Bronchiolitis, and PneumoniaDocument58 pagesLower Respiratory Tract Infections: Bronchitis, Bronchiolitis, and PneumoniaVIVEK DHADYANNo ratings yet
- Bronchitis, Pneumonia and Bronchial Asthma in ChildrenDocument82 pagesBronchitis, Pneumonia and Bronchial Asthma in Childrenstrawberry pieNo ratings yet
- Pediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentDocument43 pagesPediatric Community-Acquired Pneumonia: Causes, Symptoms & TreatmentRazel Kinette AzotesNo ratings yet
- Chapter 1Document30 pagesChapter 1Ayro Business CenterNo ratings yet
- Upper Respiratory Tract InfectionDocument3 pagesUpper Respiratory Tract Infectionmcvirgo014100% (1)
- Lower Airway DiseasesDocument70 pagesLower Airway DiseasesAavash PradhanNo ratings yet
- Bacteria Infection of The Respiratory TractDocument8 pagesBacteria Infection of The Respiratory TractChidi EmmanuelNo ratings yet
- Infeksi Saluran Napas BawahDocument54 pagesInfeksi Saluran Napas Bawahfahri somantriNo ratings yet
- Microbial Diseases of the Respiratory System: Bacteria, Viruses and FungiDocument63 pagesMicrobial Diseases of the Respiratory System: Bacteria, Viruses and Fungirandom stuffNo ratings yet
- Acute Respiratory Infections in ChildrenDocument43 pagesAcute Respiratory Infections in ChildrenAgiana PratamaNo ratings yet
- PAEDIATRICS Notes 3 Update PDFDocument69 pagesPAEDIATRICS Notes 3 Update PDFMateen ShukriNo ratings yet
- 14 Respiratory InfectionsDocument16 pages14 Respiratory InfectionsEsteban PrietoNo ratings yet
- 5 Mikrobiologi (Dr. Enny S, M.kes)Document115 pages5 Mikrobiologi (Dr. Enny S, M.kes)fitkaNo ratings yet
- Pneumonia Diagnosis and PathogenesisDocument104 pagesPneumonia Diagnosis and PathogenesissallykartikaNo ratings yet
- Microbial Diseases of The Respiratory System: Micropara-Respiratory Infectionby DR Sonnie TalaveraDocument167 pagesMicrobial Diseases of The Respiratory System: Micropara-Respiratory Infectionby DR Sonnie Talaveraone_nd_onlyuNo ratings yet
- Acute Respiratory Infection GuideDocument62 pagesAcute Respiratory Infection GuideSecret AgentNo ratings yet
- Rhino PharyngitisDocument27 pagesRhino PharyngitisinriantoNo ratings yet
- Pathophysiology and Presentation of Tuberculosis InfectionDocument5 pagesPathophysiology and Presentation of Tuberculosis InfectionFerdi StefiyanNo ratings yet
- W1 L1 URTI (Outdated)Document41 pagesW1 L1 URTI (Outdated)Anas FikriNo ratings yet
- Diseases of The Respiratory SystemDocument44 pagesDiseases of The Respiratory SystemEugenia Ceban100% (2)
- Acute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODocument29 pagesAcute Respiratory Viral Infections: Prof. S. M. Turyanitsa Dr. Karabinyosh S.ODOCTOR DanishNo ratings yet
- Acute Respiratory InfectoonDocument39 pagesAcute Respiratory InfectoonMahesa RamadhiantoNo ratings yet
- Pneumonia Symptoms and SignsDocument51 pagesPneumonia Symptoms and SignsArleen MatincaNo ratings yet
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDocument2 pagesAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoNo ratings yet
- Pneumonia: DR - Dr. Tahan P.H.,Spp.,Dtce.,Mars Fk-Uwk, 1 April 2011Document42 pagesPneumonia: DR - Dr. Tahan P.H.,Spp.,Dtce.,Mars Fk-Uwk, 1 April 2011Mimi fitrianiNo ratings yet
- Hidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkDocument52 pagesHidalgo, Rubenjie S. Dela Cruz, Anthony Jericho B. Abary, Claudine D. Tan Hoc, Anne Mei H. Oca, Renx MarkEira LopezNo ratings yet
- Evaluation and Management of Pharyngitis in Children: Treatment To Avoid Unnecessary Antibiotics For ViralDocument19 pagesEvaluation and Management of Pharyngitis in Children: Treatment To Avoid Unnecessary Antibiotics For ViralSumeet MandhanNo ratings yet
- Bronchiectasis and Lung Abscess Diagnosis and TreatmentDocument56 pagesBronchiectasis and Lung Abscess Diagnosis and TreatmentMansi GandhiNo ratings yet
- The Flu: A Guide for Prevention and TreatmentFrom EverandThe Flu: A Guide for Prevention and TreatmentRating: 5 out of 5 stars5/5 (1)
- Аcute and chronic pancreatitisDocument14 pagesАcute and chronic pancreatitisمیاں منیب احمدNo ratings yet
- Peptic UlcerDocument57 pagesPeptic Ulcerمیاں منیب احمدNo ratings yet
- BRONCHIECTASISDocument17 pagesBRONCHIECTASISمیاں منیب احمدNo ratings yet
- Diabetes MellitusDocument38 pagesDiabetes Mellitusمیاں منیب احمدNo ratings yet
- Basic LCI To High LCIDocument3 pagesBasic LCI To High LCIIonut VladNo ratings yet
- Eole Press KitDocument15 pagesEole Press KitBob AndrepontNo ratings yet
- Corporate Governance in SMEsDocument18 pagesCorporate Governance in SMEsSana DjaanineNo ratings yet
- Understanding 2006 PSAT-NMSQT ScoresDocument8 pagesUnderstanding 2006 PSAT-NMSQT ScorestacobeoNo ratings yet
- Cell Selection ReselectionDocument35 pagesCell Selection ReselectionThiaguNo ratings yet
- Scientology Abridged Dictionary 1973Document21 pagesScientology Abridged Dictionary 1973Cristiano Manzzini100% (2)
- Muv PDFDocument6 pagesMuv PDFDenisse PxndithxNo ratings yet
- Agilent Cool On-Column Operation ManualDocument42 pagesAgilent Cool On-Column Operation Manualdmcevoy1965No ratings yet
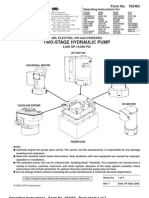
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- INVENTORY MANAGEMENT TechniquesDocument24 pagesINVENTORY MANAGEMENT TechniquesWessal100% (1)
- Openness To Experience: Intellect & Openness: Lecture Notes 8Document8 pagesOpenness To Experience: Intellect & Openness: Lecture Notes 8Danilo Pesic100% (1)
- Presentation 1Document20 pagesPresentation 1nikitakhanduja1304No ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- Oracle Unified Method (OUM) White Paper - Oracle's Full Lifecycle Method For Deploying Oracle-Based Business Solutions - GeneralDocument17 pagesOracle Unified Method (OUM) White Paper - Oracle's Full Lifecycle Method For Deploying Oracle-Based Business Solutions - GeneralAndreea Mirosnicencu100% (1)
- ChromosomesDocument24 pagesChromosomesapi-249102379No ratings yet
- Dyna 2000 LiteDocument2 pagesDyna 2000 LiteRNKNo ratings yet
- ClientsDocument7 pagesClientsLiane PanahacNo ratings yet
- A Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulDocument19 pagesA Summer Internship Project ON " To Study The Supply Chain Management On Amul Fresh Products" AT GCMMF, AmulweetrydhNo ratings yet
- Variables in Language Teaching - The Role of The TeacherDocument34 pagesVariables in Language Teaching - The Role of The TeacherFatin AqilahNo ratings yet
- 2nd QUARTER EXAMINATION IN P. E 2019-2020Document3 pages2nd QUARTER EXAMINATION IN P. E 2019-2020Lyzl Mahinay Ejercito MontealtoNo ratings yet
- Characteristics and Guidelines of PublicspaceDocument3 pagesCharacteristics and Guidelines of PublicspaceJanani SurenderNo ratings yet
- 2010 HSC Exam PhysicsDocument42 pages2010 HSC Exam PhysicsVictor345No ratings yet
- Environmental Threats Differentiated Reading Comprehension Ver 1Document20 pagesEnvironmental Threats Differentiated Reading Comprehension Ver 1Camila DiasNo ratings yet
- Multivariate Analysis Homework QuestionsDocument2 pagesMultivariate Analysis Homework Questions歐怡君No ratings yet
- List of household items for relocationDocument4 pagesList of household items for relocationMADDYNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- 3.1 C 4.5 Algorithm-19Document10 pages3.1 C 4.5 Algorithm-19nayan jainNo ratings yet
- Types of Speech StylesDocument31 pagesTypes of Speech StylesRomnick BistayanNo ratings yet
- Appliance Saver Prevents OverheatingDocument2 pagesAppliance Saver Prevents OverheatingphilipNo ratings yet
- X RayDocument16 pagesX RayMedical Physics2124No ratings yet