You might also like
- Head Trauma: Drs. Afnan Abdirahman MBBS Elrazi University General Surgery Resident (UOH/IMU)Document30 pagesHead Trauma: Drs. Afnan Abdirahman MBBS Elrazi University General Surgery Resident (UOH/IMU)DrRahma Ali HeissNo ratings yet
- Vertigo, A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandVertigo, A Simple Guide to The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
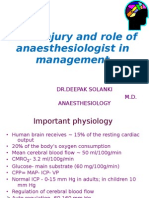
- Head Injury and Role of Anaesthesiologist in ManagementDocument38 pagesHead Injury and Role of Anaesthesiologist in ManagementDeepak SolankiNo ratings yet
- HEAD INJURY (Trauma Kepala) DR - AgusDocument53 pagesHEAD INJURY (Trauma Kepala) DR - AgusSetyo RahmanNo ratings yet
- Traumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaDocument62 pagesTraumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaRey AlwiwikhNo ratings yet
- Head InjuryDocument88 pagesHead InjuryPrisca Angelina100% (2)
- Head Injuries 2015Document41 pagesHead Injuries 2015jimmyNo ratings yet
- Head Injury Management GuideDocument58 pagesHead Injury Management GuideMuvenn KannanNo ratings yet
- Kuliah Head Injury MakasarDocument113 pagesKuliah Head Injury MakasarJerrod WilsonNo ratings yet
- Trauma and Brain InjuryDocument48 pagesTrauma and Brain Injurya20-0353-958No ratings yet
- Head InjuryDocument50 pagesHead InjuryThiagarajah RaviNo ratings yet
- Head InjuryDocument36 pagesHead InjuryNorFarah Fatin AnuarNo ratings yet
- Brain TraumaDocument32 pagesBrain Traumafrengki kobogauNo ratings yet
- Head Trauma: Types of Resulting Brain InjuryDocument6 pagesHead Trauma: Types of Resulting Brain InjuryAnjali ParajuliNo ratings yet
- Update: Management of Head InjuriesDocument38 pagesUpdate: Management of Head InjuriesWilly OematanNo ratings yet
- HEAD INJURY MANAGEMENT UPDATEDocument38 pagesHEAD INJURY MANAGEMENT UPDATERoby Aditya SuryaNo ratings yet
- Management OF Head Injury: DR Echebiri, PDocument26 pagesManagement OF Head Injury: DR Echebiri, PLuther ThengNo ratings yet
- Head Injury 2022.Document45 pagesHead Injury 2022.Alia QNo ratings yet
- Traumatic Brain Injury (TBI)Document48 pagesTraumatic Brain Injury (TBI)Alaa OmarNo ratings yet
- Dr. Tommy SP - BS - Head Trauma Webinar Dr. TMYDocument30 pagesDr. Tommy SP - BS - Head Trauma Webinar Dr. TMYOctafiani Trikartika DarimanNo ratings yet
- Head Injury AnesDocument42 pagesHead Injury Aneskenbon kenbonNo ratings yet
- Perinatal Asphyxia: For C-IDocument35 pagesPerinatal Asphyxia: For C-IYemata HailuNo ratings yet
- CBT Neurosurgery - TutorDocument24 pagesCBT Neurosurgery - Tutoramoody95No ratings yet
- Head Injury Outline of Management CDocument89 pagesHead Injury Outline of Management CPanna SahaNo ratings yet
- Head Trauma (Head Injury) : Thitinan LimchoopornwikulDocument42 pagesHead Trauma (Head Injury) : Thitinan LimchoopornwikulPasut ChangeNo ratings yet
- Approach To A Child With Coma by Dr. M. A. Rahim 2 Year PGT Paediatric MedicineDocument64 pagesApproach To A Child With Coma by Dr. M. A. Rahim 2 Year PGT Paediatric MedicineRipan SahaNo ratings yet
- Understanding Traumatic Brain InjuryDocument59 pagesUnderstanding Traumatic Brain InjuryYusfitaria AlvinaNo ratings yet
- Head Trauma: Initial Assessment and ManagementDocument38 pagesHead Trauma: Initial Assessment and Managementi wayan dediyanaNo ratings yet
- head injuryDocument39 pageshead injuryYonathan asnakeNo ratings yet
- Head Traumas: Anthony Safi Mediii Neurosurgery RotationDocument17 pagesHead Traumas: Anthony Safi Mediii Neurosurgery RotationAnthony safiNo ratings yet
- Head Trauma: Dr. Andy Wijaya, SpemDocument20 pagesHead Trauma: Dr. Andy Wijaya, SpemThomas AlbertNo ratings yet
- Head InjuryDocument34 pagesHead Injuryrxmskdkd33No ratings yet
- Thenan - Danial - AinaDocument33 pagesThenan - Danial - AinaThenan SankarNo ratings yet
- Neurosurgery Case 1Document111 pagesNeurosurgery Case 1api-3704562No ratings yet
- ApproachtocomaDocument65 pagesApproachtocomantnquynhproNo ratings yet
- 3 NeurologicalDocument57 pages3 NeurologicalrakeshghonasagiNo ratings yet
- Head Trauma Guide: Concussions, Hematomas & CT InterpretationDocument193 pagesHead Trauma Guide: Concussions, Hematomas & CT InterpretationhanimozaghiNo ratings yet
- Understanding Brain Death, Coma, and StrokeDocument21 pagesUnderstanding Brain Death, Coma, and StrokeDrGasnasNo ratings yet
- Head InjuryDocument64 pagesHead Injurybuttashly125No ratings yet
- Head Trauma Chapter 6Document43 pagesHead Trauma Chapter 6Aray Al-AfiqahNo ratings yet
- Head Trauma: Dr. Nasir Lamhot, Sp. BSDocument31 pagesHead Trauma: Dr. Nasir Lamhot, Sp. BSYohannes KurniawanNo ratings yet
- Head TraumaDocument54 pagesHead TraumaVidelia ArlitaNo ratings yet
- NEUROLOGICALDocument3 pagesNEUROLOGICALRizMarie100% (4)
- EPIDURAL HAEMATOMA GUIDEDocument65 pagesEPIDURAL HAEMATOMA GUIDESitha ChristineNo ratings yet
- Brain DeathDocument43 pagesBrain Deathanimesh pandaNo ratings yet
- Monitor blood glucose levels closely and maintain euglycemiaDocument74 pagesMonitor blood glucose levels closely and maintain euglycemiaLuther ThengNo ratings yet
- Craniocerebral Injury/ Head InjuryDocument36 pagesCraniocerebral Injury/ Head InjurySamjhana GautamNo ratings yet
- Cedera Kepala Dan Otak: Dr. Isnaniah, Sp. S Bagian Saraf Fkik UntadDocument91 pagesCedera Kepala Dan Otak: Dr. Isnaniah, Sp. S Bagian Saraf Fkik UntadSiwa MerthadinataNo ratings yet
- Unit 2.2 (C) Trauma Head InjuryDocument39 pagesUnit 2.2 (C) Trauma Head Injurysymonlangisi354No ratings yet
- Head Injury 1Document87 pagesHead Injury 1akshay mohanNo ratings yet
- Management of Head Injuries (Open and ClosedDocument48 pagesManagement of Head Injuries (Open and ClosedAsmahan AliNo ratings yet
- Cerebral ConcussionDocument4 pagesCerebral Concussionnur_shakirin0% (1)
- CPP Monitoring for Cerebral Perfusion AssessmentDocument131 pagesCPP Monitoring for Cerebral Perfusion AssessmentEMBER MARIE SAYMANNo ratings yet
- Tbi Case PresentationDocument22 pagesTbi Case PresentationNinaNo ratings yet
- 5A. Traumatic Brain InjuriesDocument242 pages5A. Traumatic Brain InjuriesMajed AlamiNo ratings yet
- 9 5神經系統Document59 pages9 5神經系統陳姿螢No ratings yet
- Brain Injury Dr. Shema Dr. MuyimboDocument58 pagesBrain Injury Dr. Shema Dr. MuyimboTIMOTHY MUYIMBONo ratings yet
- TBI FinalDocument28 pagesTBI Finalawais mpNo ratings yet
- Askep ANC ZAKFAR EVENDYDocument19 pagesAskep ANC ZAKFAR EVENDYzakfar evendyNo ratings yet
- Vidio Summary - 215070209111031 - Lucy Puspita SeptianaDocument3 pagesVidio Summary - 215070209111031 - Lucy Puspita Septianazakfar evendyNo ratings yet
- Assessing a Brain Tumor Originally Thought to be Anxiety-Related HyperventilationDocument1 pageAssessing a Brain Tumor Originally Thought to be Anxiety-Related Hyperventilationzakfar evendyNo ratings yet
- 2016 - 13 - 8 ACIPC Position Preoperative Skin AntisepsisDocument6 pages2016 - 13 - 8 ACIPC Position Preoperative Skin Antisepsiszakfar evendyNo ratings yet
- Intracranial SurgeryDocument12 pagesIntracranial Surgeryzakfar evendyNo ratings yet
- 2016 - 13 - 8 ACIPC Position Preoperative Skin AntisepsisDocument6 pages2016 - 13 - 8 ACIPC Position Preoperative Skin Antisepsiszakfar evendyNo ratings yet
- ETHICON Encyclopedia of Knots (Noduri Chirurgicale PDFDocument49 pagesETHICON Encyclopedia of Knots (Noduri Chirurgicale PDFoctav88No ratings yet
- Imaging Findings and Clinical Correlation: Cerebral Herniation SyndromesDocument64 pagesImaging Findings and Clinical Correlation: Cerebral Herniation SyndromessridharNo ratings yet
- P1Document12 pagesP1Roykedona Lisa TrixieNo ratings yet
- Blumenfeld Neuroanatomy Ch. 5 SummaryDocument5 pagesBlumenfeld Neuroanatomy Ch. 5 SummaryMeeraNo ratings yet
- Pentagon Review Royal PentagonDocument33 pagesPentagon Review Royal PentagonRichard Ines Valino99% (70)
- ED Burr HolesDocument4 pagesED Burr HolesGebrie DinkayehuNo ratings yet
- Modified Morbid Anatomy PracticalDocument65 pagesModified Morbid Anatomy PracticalEbenezer GodwinNo ratings yet
- Deepak Jaiswal V Oriental Insurance'Document3 pagesDeepak Jaiswal V Oriental Insurance'Yashasvi SharmaNo ratings yet
- Brain HerniationDocument40 pagesBrain HerniationAnusha VergheseNo ratings yet
- Usmle Board Review Step 1Document357 pagesUsmle Board Review Step 1pereje7067% (3)
- NEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFDocument3 pagesNEURO2 3.05 Neurosurgical Management of Stroke and CNS Infection - Dr. Domingo PDFPatricia Nicole AlcarazNo ratings yet
- NeuropathologyDocument67 pagesNeuropathologyEmanuelNo ratings yet
- Intracranial Pressure Monitoring ReportingDocument26 pagesIntracranial Pressure Monitoring ReportingMary Johna PancrudoNo ratings yet
- Plum and Posner's Diagnosis of Stupor and ComaDocument416 pagesPlum and Posner's Diagnosis of Stupor and Comakikotido8100% (1)
- Concept Map TBIDocument2 pagesConcept Map TBIraquel maniego67% (3)
- Med SurDocument107 pagesMed Surapi-239934742No ratings yet
- Subdural HematomaDocument8 pagesSubdural HematomaaaronmanullangNo ratings yet
- Brain herniation causes, types and symptomsDocument5 pagesBrain herniation causes, types and symptomsOktafiani tri AnandaNo ratings yet
- NCM 116 - Nursing Care of Patients With Neurologic DysfunctionDocument11 pagesNCM 116 - Nursing Care of Patients With Neurologic DysfunctionRigel Kent C. TobiasNo ratings yet
- Full Autopsy Released in Death of Kyler PresnellDocument9 pagesFull Autopsy Released in Death of Kyler PresnellKrystyna May67% (3)
- Shaukat Khanum Memorial Cancer Hospital & Research Centre: CPT: History: Mri Brain Without ContrastDocument1 pageShaukat Khanum Memorial Cancer Hospital & Research Centre: CPT: History: Mri Brain Without ContrastHina KhanNo ratings yet
- Neuro ICUDocument11 pagesNeuro ICUBatch V Med 2 SY 21-22No ratings yet
- Stupor and Coma in AdultsDocument14 pagesStupor and Coma in AdultsElena Chitoiu100% (1)
- Neuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansDocument29 pagesNeuroscience Ii: Summary: Nationality (Will Tell You Incidence, For Example, AsiansAngelaTrinidad100% (2)
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshNo ratings yet
- Medical Surgical Nursing With MnemonicsDocument111 pagesMedical Surgical Nursing With MnemonicsChernobyle Tolentino BattadNo ratings yet
- Anaesthesia & Intensive Care: Short Answer QuestionsDocument53 pagesAnaesthesia & Intensive Care: Short Answer QuestionsPaola FgmNo ratings yet
- Trauma For FmgeDocument17 pagesTrauma For FmgeMuhammad ZeeshanNo ratings yet
- Everything You Need to Know About Breast ImagingDocument21 pagesEverything You Need to Know About Breast ImagingOmar Nayef Taani83% (6)
- Neurosensory Disorders 22306Document14 pagesNeurosensory Disorders 22306bekbekk cabahugNo ratings yet
- Head Trauma PDFDocument66 pagesHead Trauma PDFnuraNo ratings yet