You might also like
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Diabetes Study GuideDocument4 pagesDiabetes Study GuideNicole Brassington0% (1)
- Diabetes Management ATIDocument15 pagesDiabetes Management ATIJessica ChirinoNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Diabetes MellitusDocument16 pagesDiabetes MellitusApril Joy V. QuinoNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Pharmacology Review NotesDocument24 pagesPharmacology Review NotescampbellqueenNo ratings yet
- NUR 201 Diabetes PowerpointDocument53 pagesNUR 201 Diabetes PowerpointSaad MotawéaNo ratings yet
- DZIELSKA MARIA 1996 Hypatia of Alexandria (Harvard University Press)Document180 pagesDZIELSKA MARIA 1996 Hypatia of Alexandria (Harvard University Press)ivory2011100% (3)
- NUR 377 Advanced Medical Surgical Nursing vSim Course Point PharmacologyDocument5 pagesNUR 377 Advanced Medical Surgical Nursing vSim Course Point PharmacologyMichelle Pinkhasova100% (3)
- Blood Glucose-Insulin Administration-Study GuideDocument8 pagesBlood Glucose-Insulin Administration-Study GuideChandra MuraliNo ratings yet
- HypoglycemiaDocument42 pagesHypoglycemiaseem neemNo ratings yet
- Diabetes, DKA, HHNS NCLEX REVIEWDocument10 pagesDiabetes, DKA, HHNS NCLEX REVIEWMonica JubaneNo ratings yet
- On The Metres of Poetry and Related Matters According To AristotleDocument61 pagesOn The Metres of Poetry and Related Matters According To AristotleBart MazzettiNo ratings yet
- HSC Blade Runner & Frankenstein EssayDocument2 pagesHSC Blade Runner & Frankenstein EssayAsha Forsyth100% (1)
- Building Machine Learning Systems With Python - Second Edition - Sample ChapterDocument32 pagesBuilding Machine Learning Systems With Python - Second Edition - Sample ChapterPackt PublishingNo ratings yet
- Hypoglycemia: Presented by Farse GhabayenDocument11 pagesHypoglycemia: Presented by Farse GhabayenFares G. Ghabayen100% (2)
- Diabetes ExamDocument7 pagesDiabetes ExambennybuffetNo ratings yet
- Ms DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesDocument9 pagesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesMs DiabetesLariza LopegaNo ratings yet
- Diabetes Exam With AnswersDocument12 pagesDiabetes Exam With AnswersJed TumaliwanNo ratings yet
- Pre TestDocument5 pagesPre TestZhyraine Iraj D. CaluzaNo ratings yet
- Endocrine SystemDocument21 pagesEndocrine SystemMona MahfouzNo ratings yet
- Types of DM:-: - DefinitionDocument23 pagesTypes of DM:-: - DefinitionKarrar KarrarNo ratings yet
- Complications of Insulin TherapyDocument16 pagesComplications of Insulin TherapyIngrid NicolasNo ratings yet
- Common Endocrine Disorders: Iril I. Panes, RN, MANDocument63 pagesCommon Endocrine Disorders: Iril I. Panes, RN, MANJona Phie Domingo MonteroNo ratings yet
- Critical Thinking Exercise 10Document3 pagesCritical Thinking Exercise 10Hope SerquiñaNo ratings yet
- Antidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyDocument18 pagesAntidiabetic Drugs: DR Nagwa Nour EL Din Assistant Professor PharmacologyMohamed AlaaNo ratings yet
- Pharm Quiz 1Document59 pagesPharm Quiz 1Anonymous vXOM1Wxt100% (1)
- 2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportDocument2 pages2022 Oxford Handbook of Anaesthesia Oxford Press 5th Edition ExportHany Elbarougy0% (1)
- Recent Advances in Therapy of DiabetesDocument62 pagesRecent Advances in Therapy of DiabetesMohd KhatibNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- CH 39 Anaesthesia and Diabetes MellitusDocument6 pagesCH 39 Anaesthesia and Diabetes MellitusChristian LeepoNo ratings yet
- DM Presentation NewDocument44 pagesDM Presentation NewKipz JonsNo ratings yet
- DiabetesDocument42 pagesDiabetesSteph VistalNo ratings yet
- Anti-Diabetic Drugs GuideDocument39 pagesAnti-Diabetic Drugs GuideNurul Mursyidah ZakariaNo ratings yet
- NR 325 Diabetes Power-Student Copy1118Document39 pagesNR 325 Diabetes Power-Student Copy1118John MixerNo ratings yet
- Managing Diabetes Complications and EmergenciesDocument21 pagesManaging Diabetes Complications and EmergenciesHanna BaddiriNo ratings yet
- Cdho Assignment 2 Type 1 DiabetesDocument10 pagesCdho Assignment 2 Type 1 Diabetesapi-596913754No ratings yet
- Compilation P2 MS2 PDFDocument31 pagesCompilation P2 MS2 PDFGwenn SalazarNo ratings yet
- Gestational Diabetes Mellitus DefinitionDocument4 pagesGestational Diabetes Mellitus DefinitionTempoNo ratings yet
- Antidiabetic Agents GuideDocument19 pagesAntidiabetic Agents GuideJames SoeNo ratings yet
- Insulin AdministrationDocument8 pagesInsulin AdministrationskybluealiNo ratings yet
- InsulinDocument4 pagesInsulinHa Zizzle100% (1)
- Disorders in the Pancreas and Ovaries: Diagnosis and TreatmentDocument49 pagesDisorders in the Pancreas and Ovaries: Diagnosis and TreatmentwyneNo ratings yet
- Insulin, Oral Hypoglycemic Agents-1Document23 pagesInsulin, Oral Hypoglycemic Agents-1IbrahimNo ratings yet
- Nursing Considerations for Patients with DiabetesDocument7 pagesNursing Considerations for Patients with Diabeteslanguha NgatiNo ratings yet
- DiabetesmellitusDocument24 pagesDiabetesmellitusSania SaeedNo ratings yet
- Drugs Used to Treat Diabetes Mellitus: Insulin and Oral AgentsDocument37 pagesDrugs Used to Treat Diabetes Mellitus: Insulin and Oral AgentsjisooNo ratings yet
- What Is DiabetesDocument9 pagesWhat Is Diabeteskdubb90No ratings yet
- Diabetes Mellitus IIDocument10 pagesDiabetes Mellitus IIaa zzNo ratings yet
- Pharmacology LectureDocument6 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Assignment (Diabetes)Document9 pagesAssignment (Diabetes)Wynne EnglatieraNo ratings yet
- MS3 Review NotesDocument11 pagesMS3 Review NotesPaul Anthony LoricaNo ratings yet
- Module 9 ElaborateDocument6 pagesModule 9 ElaborateTrishaNo ratings yet
- The Essential Role of Insulin in Diabetes ManagementDocument9 pagesThe Essential Role of Insulin in Diabetes ManagementAbdul SamadNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Guideline, Management of HypoglycemiaDocument5 pagesGuideline, Management of HypoglycemianellieauthorNo ratings yet
- Managing diabetes: clinical manifestations, treatment, and prevention of complicationsDocument40 pagesManaging diabetes: clinical manifestations, treatment, and prevention of complicationsreza dehghaniNo ratings yet
- Diabetes MellitusDocument24 pagesDiabetes MellitusNiña Ricci MtflcoNo ratings yet
- Type I Diabetes Mellitus Management in The Athletic PopulationDocument22 pagesType I Diabetes Mellitus Management in The Athletic PopulationRitesh NetamNo ratings yet
- Gds137 Slide Diabetes Melitus Type 1Document31 pagesGds137 Slide Diabetes Melitus Type 1viscabarca543No ratings yet
- Note Exam 2Document7 pagesNote Exam 2Jamie BywaterNo ratings yet
- DM QuestionsDocument8 pagesDM QuestionsRegiever SalvanteNo ratings yet
- Research Paper 1 3 Revised Date Mar 3Document42 pagesResearch Paper 1 3 Revised Date Mar 3Marielle CabanbanNo ratings yet
- ABC 2021 Chapter 4 EditDocument9 pagesABC 2021 Chapter 4 EditMarielle CabanbanNo ratings yet
- Graves Disease CasanesDocument8 pagesGraves Disease CasanesMarielle CabanbanNo ratings yet
- Personality Disorders FinalDocument137 pagesPersonality Disorders FinalMarielle CabanbanNo ratings yet
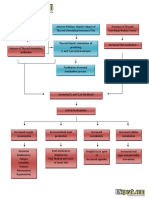
- Pathophysiology of HyperthyroidismDocument1 pagePathophysiology of HyperthyroidismMarielle CabanbanNo ratings yet
- PUD GordonsDocument13 pagesPUD GordonsMarielle CabanbanNo ratings yet
- Pathophysiology of HyperthyroidismDocument1 pagePathophysiology of HyperthyroidismMarielle CabanbanNo ratings yet
- PUD GordonsDocument13 pagesPUD GordonsMarielle CabanbanNo ratings yet
- HOW Katipunan Became A Catalyst: Marielle O. CabanbanDocument6 pagesHOW Katipunan Became A Catalyst: Marielle O. CabanbanMarielle CabanbanNo ratings yet
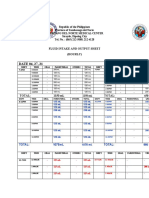
- Zamboanga del Norte Medical Center fluid intake output sheetDocument3 pagesZamboanga del Norte Medical Center fluid intake output sheetMarielle CabanbanNo ratings yet
- Supreme Court Ruling on Missing Court RecordsDocument7 pagesSupreme Court Ruling on Missing Court RecordsApr CelestialNo ratings yet
- Gujarat Technological University Subject: VLSI Technology & Design Code:2161101 Topic - 3 - MOS TransistorDocument122 pagesGujarat Technological University Subject: VLSI Technology & Design Code:2161101 Topic - 3 - MOS Transistorbakoliy218No ratings yet
- Partner With Rittal: It's Easy To Become A Rittal PartnerDocument10 pagesPartner With Rittal: It's Easy To Become A Rittal PartnerBhanu Uday SinghNo ratings yet
- Math 7 - Week 2 SummativeDocument1 pageMath 7 - Week 2 SummativeBrian Mary0% (1)
- 028 - Chapter 6 - L20 PDFDocument11 pages028 - Chapter 6 - L20 PDFRevathiNo ratings yet
- Deadlocks in OSDocument2 pagesDeadlocks in OS47 Bhushan BariNo ratings yet
- Beyond The Wall - The Village Hero Character PlaybookDocument4 pagesBeyond The Wall - The Village Hero Character Playbookmagic_fyodorNo ratings yet
- Cryosurgery and ElectrosurgeryDocument51 pagesCryosurgery and ElectrosurgeryVeerabhadra RadhakrishnaNo ratings yet
- CMRIT R18 Syllabus ME PDFDocument142 pagesCMRIT R18 Syllabus ME PDFMaddipudi RamakrishnaNo ratings yet
- Gang Rape Jokes by ViceralDocument1 pageGang Rape Jokes by ViceralimmissgeniusNo ratings yet
- N039-N040 Rejano Nursing Care PlanDocument3 pagesN039-N040 Rejano Nursing Care PlanBianca Marithè RejanoNo ratings yet
- NEW GENERATION INTERNATIONAL SCHOOL SECOND UNIT TESTDocument4 pagesNEW GENERATION INTERNATIONAL SCHOOL SECOND UNIT TESTElmy ARNo ratings yet
- SIOP Lesson PlanDocument6 pagesSIOP Lesson PlanSmithRichardL1988100% (3)
- Foreigners, Pharaonic Egypt: Kate LiszkaDocument3 pagesForeigners, Pharaonic Egypt: Kate LiszkaSongNo ratings yet
- Biochemistry of InflamationDocument45 pagesBiochemistry of Inflamationmichot feleguNo ratings yet
- Spare Order 28.03Document27 pagesSpare Order 28.03Ankit AgarwalNo ratings yet
- Repaso 5to Grado 3°trimestreDocument25 pagesRepaso 5to Grado 3°trimestreFany BalderramaNo ratings yet
- 07 Part of Speech ActivitiesDocument6 pages07 Part of Speech ActivitiesLorraine UnigoNo ratings yet
- Skema Pppa Kimia k2 2014 (Set 1)Document10 pagesSkema Pppa Kimia k2 2014 (Set 1)Siva Guru0% (1)
- Curriculum Vitae: Radhey ShyamDocument3 pagesCurriculum Vitae: Radhey ShyamGaurav SinghNo ratings yet
- Bandingan Ko Maana Simba Ko IslamDocument7 pagesBandingan Ko Maana Simba Ko IslamJohari AbubacarNo ratings yet
- History PPT 1Document24 pagesHistory PPT 1Akash SharmaNo ratings yet
- Macro PerspectiveDocument3 pagesMacro PerspectiveMARITONI MEDALLANo ratings yet
- SF PLT Managing Picklists Admin PDFDocument38 pagesSF PLT Managing Picklists Admin PDFHiNo ratings yet
- Republic of the Philippines v. Marcos: 9th Circuit Affirms Preliminary Injunction Against Disposing AssetsDocument18 pagesRepublic of the Philippines v. Marcos: 9th Circuit Affirms Preliminary Injunction Against Disposing AssetsAaron CariñoNo ratings yet
- SafeNet Ikey4000 PB (En) WebDocument2 pagesSafeNet Ikey4000 PB (En) WebbasharaccountNo ratings yet