You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4th Year Multiple PregnancyDocument57 pages4th Year Multiple PregnancyKingsley Calex100% (2)
- Demonstration On NALSDocument20 pagesDemonstration On NALSMary MenuNo ratings yet
- Cesarean Delivery Case Presentation ConceptualDocument57 pagesCesarean Delivery Case Presentation ConceptualHope Serquiña67% (3)
- MCN Book ProjectDocument74 pagesMCN Book ProjectRonnie De Vera IINo ratings yet
- New Ballard ScoreDocument39 pagesNew Ballard ScoreJAMES ROD MARINDUQUENo ratings yet
- NCM 107 RLE Module 2 Nov 16 18 2020Document34 pagesNCM 107 RLE Module 2 Nov 16 18 2020mirai desuNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras Ali100% (1)
- Family Planning: By:-Dr. Addis GebruDocument69 pagesFamily Planning: By:-Dr. Addis GebrutareNo ratings yet
- MalpresentationDocument37 pagesMalpresentationLovely SarangiNo ratings yet
- Instrument of NormalDocument17 pagesInstrument of NormalEdraline Lumawig100% (2)
- Female Genital CuttingDocument15 pagesFemale Genital CuttingtareNo ratings yet
- Research Proposal UCUDocument38 pagesResearch Proposal UCUKamira Sulait Kyepa100% (1)
- Episiotomy: Dr. Fekadu R (MD) November, 2012/19Document11 pagesEpisiotomy: Dr. Fekadu R (MD) November, 2012/19tareNo ratings yet
- Antenatal Care: By: Dr. Addis GDocument40 pagesAntenatal Care: By: Dr. Addis GtareNo ratings yet
- Prelabor Rupture of Membranes (PROM) : DR Yonas GDocument19 pagesPrelabor Rupture of Membranes (PROM) : DR Yonas GtareNo ratings yet
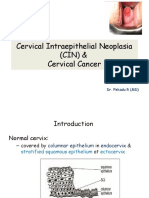
- Cervical Intraepithelial Neoplasia (CIN) & Cervical Cancer: Dr. Fekadu R (MD)Document33 pagesCervical Intraepithelial Neoplasia (CIN) & Cervical Cancer: Dr. Fekadu R (MD)tareNo ratings yet
- Abnormal Uterine BleedingDocument37 pagesAbnormal Uterine BleedingtareNo ratings yet
- Preterm Labor and DeliveryDocument19 pagesPreterm Labor and DeliverytareNo ratings yet
- Female Genital Mutilation: Definition Prevalence Classification Complications (Short Term & Long Term)Document13 pagesFemale Genital Mutilation: Definition Prevalence Classification Complications (Short Term & Long Term)tareNo ratings yet
- Antenatal Care (ANC)Document77 pagesAntenatal Care (ANC)tareNo ratings yet
- Reaction IntermediatesDocument42 pagesReaction IntermediatestareNo ratings yet
- General Pharmacology 2013Document403 pagesGeneral Pharmacology 2013tareNo ratings yet
- Wolkite University College of Engineering and Technology Department of Food Process EngineeringDocument27 pagesWolkite University College of Engineering and Technology Department of Food Process EngineeringtareNo ratings yet
- Chapter Two Chapter Two: Ideal - Batch and Semi - Batch Reactors DesignDocument21 pagesChapter Two Chapter Two: Ideal - Batch and Semi - Batch Reactors DesigntareNo ratings yet
- Food Process Engineering Department: Project Title: Extraction and Characterization of Oil From Mango SeedDocument24 pagesFood Process Engineering Department: Project Title: Extraction and Characterization of Oil From Mango SeedtareNo ratings yet
- Human Computer Interaction: Wolkite University Department of Software EngineeringDocument120 pagesHuman Computer Interaction: Wolkite University Department of Software EngineeringtareNo ratings yet
- Mass Transfer Unit Operations: Cheg 3114Document34 pagesMass Transfer Unit Operations: Cheg 3114tareNo ratings yet
- Addis Ababa Science and Technology UniversityDocument20 pagesAddis Ababa Science and Technology UniversitytareNo ratings yet
- Kuma Endale ThesisDocument51 pagesKuma Endale ThesistareNo ratings yet
- PMTCT: Ayana Benti (BSC, MSCN,) Wolkite University Department of NursingDocument59 pagesPMTCT: Ayana Benti (BSC, MSCN,) Wolkite University Department of NursingtareNo ratings yet
- Mass Transfer Unit Operations: Cheg 3114Document43 pagesMass Transfer Unit Operations: Cheg 3114tareNo ratings yet
- Reven Lex Magdaluyo Representative: Mr. John B. Ituralde. JR Humanities and Social SciencesDocument1 pageReven Lex Magdaluyo Representative: Mr. John B. Ituralde. JR Humanities and Social SciencesRaisean Lee AmarNo ratings yet
- Lamaze Early Labor InfographicDocument1 pageLamaze Early Labor Infographicionela stoicaNo ratings yet
- 1 Introduction - Domicile & Residence1Document2 pages1 Introduction - Domicile & Residence1francisNo ratings yet
- 30 - Contracted Pelvis and Cephalopelvic DisproportionDocument28 pages30 - Contracted Pelvis and Cephalopelvic Disproportiondr_asaleh93% (14)
- Ob Case StudyDocument3 pagesOb Case StudyDyriane PagsolinganNo ratings yet
- Anemia MaternityDocument5 pagesAnemia MaternityBonaventura Ahardiansyah BoNo ratings yet
- Repo File 125509 20211008 113541.DATAPENELITIANDocument63 pagesRepo File 125509 20211008 113541.DATAPENELITIANMuhamad Vanny OntaluNo ratings yet
- Strategic Objective 1Document3 pagesStrategic Objective 1Zebedee Agric BaoNo ratings yet
- Sap IdDocument1 pageSap IdMandy NoorNo ratings yet
- OB Case Studies - Fetal Monitoring-1Document2 pagesOB Case Studies - Fetal Monitoring-1Yalante BellNo ratings yet
- 40 Reasons To Go The Full 40 2022version EnglishDocument1 page40 Reasons To Go The Full 40 2022version EnglishGururaj kulkarniNo ratings yet
- JGWH - Ms.id.555623 1 KirimDocument6 pagesJGWH - Ms.id.555623 1 KirimBaiq Bunga Citra PratiwiNo ratings yet
- Problems With The PassageDocument13 pagesProblems With The PassageMaria Theresa BuscasNo ratings yet
- Gestational Hypertension and Preeclampsia ACOG.44Document4 pagesGestational Hypertension and Preeclampsia ACOG.44Daniela Vallejo AriasNo ratings yet
- Revista CienciaDocument126 pagesRevista CienciaMario SantayanaNo ratings yet
- Prevalence and Risk Factors For Symptoms of Common MentalDocument7 pagesPrevalence and Risk Factors For Symptoms of Common MentalZakkiyatus ZainiyahNo ratings yet
- The RH Factor: How It Can Affect Your PregnancyDocument3 pagesThe RH Factor: How It Can Affect Your PregnancyTedd CamilingNo ratings yet
- Psychology Core Concepts 7th Edition Zimbardo Test BankDocument78 pagesPsychology Core Concepts 7th Edition Zimbardo Test Banketiolatepuff33tj100% (28)
- Gynecological ProblemDocument40 pagesGynecological Problemannu panchalNo ratings yet
- Should Abortion Be Legalised?Document4 pagesShould Abortion Be Legalised?Eershad Muhammad GunessNo ratings yet