You might also like
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
- Health and Safety Standards in D&TDocument9 pagesHealth and Safety Standards in D&TAnnie HawkinsNo ratings yet
- 1.2 POWERPOINT History of ForensicsDocument23 pages1.2 POWERPOINT History of ForensicsSilay Parole & ProbationNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- Hazards of Nitrogen AsphyxiationDocument10 pagesHazards of Nitrogen AsphyxiationRaja Senthil NathanNo ratings yet
- Food Safety Plan For CateringDocument80 pagesFood Safety Plan For CateringNghia Khang100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Grief & Grieving ProcessDocument39 pagesGrief & Grieving Processelmerconde100% (4)
- Procurement Management SlidesDocument14 pagesProcurement Management SlidesManojNo ratings yet
- Bronchial AsthmaDocument39 pagesBronchial AsthmaSaeed mohamed100% (1)
- Standard Form Contract GuideDocument24 pagesStandard Form Contract GuideManojNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Bidding and Contract DocumentDocument45 pagesBidding and Contract DocumentManojNo ratings yet
- Albendazole Drug StudyDocument6 pagesAlbendazole Drug StudyKristel Diane RidaoNo ratings yet
- Management of patients with meningitis and encephalitisDocument71 pagesManagement of patients with meningitis and encephalitisSachin DwivediNo ratings yet
- Case Study On MigraineDocument18 pagesCase Study On MigraineAbin PNo ratings yet
- Doxofylline: D 400 MG TabletsDocument33 pagesDoxofylline: D 400 MG TabletsBibek Singh Mahat100% (2)
- Meropenem: Antibiotic ClassDocument2 pagesMeropenem: Antibiotic ClassAynshbNo ratings yet
- Bronchial Asthma (1) SKDocument24 pagesBronchial Asthma (1) SKSafoora RafeeqNo ratings yet
- Patient Case StudyDocument26 pagesPatient Case StudyDinesh BanerjeeNo ratings yet
- NCP KoDocument1 pageNCP Kojiellianemae100% (1)
- Drug StudyDocument2 pagesDrug Studymegreen GamingNo ratings yet
- Antiemetic Drug - PresentationDocument14 pagesAntiemetic Drug - PresentationYue Chen100% (1)
- 02 Bronchial Asthma Circ 2018-2019Document15 pages02 Bronchial Asthma Circ 2018-2019Mooha Alanzy100% (1)
- On Dan Set RonDocument1 pageOn Dan Set Ronzepoli_zepoly6232No ratings yet
- Drug Indication Action Side Effects and Adverse Reaction Nursing ConsiderationDocument8 pagesDrug Indication Action Side Effects and Adverse Reaction Nursing Considerationkier khierNo ratings yet
- Open FractureDocument9 pagesOpen FractureAnnyl LaurelNo ratings yet
- BibliographyDocument2 pagesBibliographyMahesh T MadhavanNo ratings yet
- 8 PathoDocument2 pages8 PathoKris LingadNo ratings yet
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- POST PARTUM HEMORRHAGE: CAUSES, SIGNS, MANAGEMENTDocument38 pagesPOST PARTUM HEMORRHAGE: CAUSES, SIGNS, MANAGEMENTnyangaraNo ratings yet
- Targocid PDFDocument2 pagesTargocid PDFwahyu agung yuwonoNo ratings yet
- Urinalysis Procedure & ResultsDocument6 pagesUrinalysis Procedure & ResultsbobtagubaNo ratings yet
- MorphineDocument3 pagesMorphineAizat KamalNo ratings yet
- Scribd 020922 Case Study-Oncology A&kDocument2 pagesScribd 020922 Case Study-Oncology A&kKellie DNo ratings yet
- USC Case 04 - SinusitisDocument9 pagesUSC Case 04 - SinusitisDisti Damelia SebayangNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- Ongoing AppraisalDocument2 pagesOngoing AppraisalLouisa Marie MirandaNo ratings yet
- Nursing Care Plan Impaired Gas ExchangeDocument1 pageNursing Care Plan Impaired Gas ExchangeKarylle PetilNo ratings yet
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- Lasilactone PI 201801Document9 pagesLasilactone PI 201801Shivam GuptaNo ratings yet
- BibliographyDocument10 pagesBibliographySourav Kumar PatraNo ratings yet
- TAHBSO ReportDocument4 pagesTAHBSO ReportsachiiMeNo ratings yet
- Chronic GastritisDocument37 pagesChronic GastritisBondu Babu007No ratings yet
- Osteomalacia Care Plan/OthersDocument11 pagesOsteomalacia Care Plan/OthersJill Jackson, RNNo ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- Client Assessment BasicsDocument56 pagesClient Assessment Basicsdanny_ng080% (1)
- Hydronephrosis Fred LuceDocument69 pagesHydronephrosis Fred LuceKMNo ratings yet
- What Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistDocument12 pagesWhat Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistLidiaAMonroyRNo ratings yet
- Au Di Minor Case Study Myasthenia GravisDocument17 pagesAu Di Minor Case Study Myasthenia Gravisapi-301816885No ratings yet
- Case Report Chronic OsteomyelitisDocument34 pagesCase Report Chronic OsteomyelitisNardine Roslan100% (1)
- Thyroid Lobectomy and IsthmusectomyDocument12 pagesThyroid Lobectomy and IsthmusectomyAgustina100% (1)
- Oxygen Terapi Dan PrinsipelDocument16 pagesOxygen Terapi Dan PrinsipelAmrita KaurNo ratings yet
- Drug StudyDocument40 pagesDrug StudyLyka Milo AvilaNo ratings yet
- 13 Levels of AssessmentDocument11 pages13 Levels of AssessmentCatherine Cayda dela Cruz-BenjaminNo ratings yet
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- Case NarrativeDocument3 pagesCase NarrativeRoeder Max PangramuyenNo ratings yet
- Background: Viral Mumps InfectionDocument5 pagesBackground: Viral Mumps InfectionAgustin UyNo ratings yet
- Drug Study - CaseDocument9 pagesDrug Study - CaseMay EvelynNo ratings yet
- Post-op-Case-Conference-DM FootDocument44 pagesPost-op-Case-Conference-DM FootShereen DS Lucman100% (1)
- Epilepsy CaseDocument17 pagesEpilepsy CaseSuresh ThanneruNo ratings yet
- Drug Study Pyrantel & CefuroximeDocument2 pagesDrug Study Pyrantel & CefuroximeMikhael Briones ApasNo ratings yet
- Bukidnon State University: Endorsement Sheet Student Patient IVF Diet Medications Doctor's OrdersDocument1 pageBukidnon State University: Endorsement Sheet Student Patient IVF Diet Medications Doctor's Ordersrexinne noahNo ratings yet
- Kristia Carpio Pulmonary TuberculosisDocument31 pagesKristia Carpio Pulmonary TuberculosiskisNo ratings yet
- Osteoarthritis 1583-170210113823Document34 pagesOsteoarthritis 1583-170210113823Angelic khanNo ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- TUBERCULOSISDocument16 pagesTUBERCULOSISPankaj MandalNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
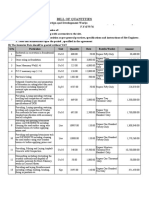
- BILL OF QUANTITIESDocument23 pagesBILL OF QUANTITIESManojNo ratings yet
- Bid Document 1Document132 pagesBid Document 1ManojNo ratings yet
- Work Order FormatDocument1 pageWork Order FormatManojNo ratings yet
- Letter of AcceptanceDocument1 pageLetter of AcceptanceManojNo ratings yet
- Contract Agreement FormatDocument1 pageContract Agreement FormatManojNo ratings yet
- Letter of IntentDocument1 pageLetter of IntentManojNo ratings yet
- Studies on Properties of TMT Steels for Structural ApplicationsDocument5 pagesStudies on Properties of TMT Steels for Structural ApplicationsManojNo ratings yet
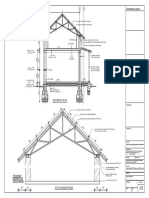
- Report-Metal Truss in Attic - FinalDocument43 pagesReport-Metal Truss in Attic - FinalManojNo ratings yet
- Advance Module Unit 7 Infectious DiseasesDocument55 pagesAdvance Module Unit 7 Infectious DiseasesManojNo ratings yet
- Metal Truss With AtticDocument2 pagesMetal Truss With AtticManojNo ratings yet
- Advance Module Unit 5 Anti Microbial and Multi Drug Resistant OrganismDocument39 pagesAdvance Module Unit 5 Anti Microbial and Multi Drug Resistant OrganismManojNo ratings yet
- Blood Sugar Management in IcuDocument10 pagesBlood Sugar Management in IcuManojNo ratings yet
- Corrosion Behaviour of TMTDocument8 pagesCorrosion Behaviour of TMTManojNo ratings yet
- Studies on Properties of TMT Steels for Structural ApplicationsDocument5 pagesStudies on Properties of TMT Steels for Structural ApplicationsManojNo ratings yet
- Construction Materials INDUSTRY NOWDocument10 pagesConstruction Materials INDUSTRY NOWManojNo ratings yet
- Room 1 9'-0"X9'-0" Room 2 9'-0"X9'-0": S.No Symbol Size NumberDocument3 pagesRoom 1 9'-0"X9'-0" Room 2 9'-0"X9'-0": S.No Symbol Size NumberManojNo ratings yet
- Corrosion Behaviour of TMTDocument8 pagesCorrosion Behaviour of TMTManojNo ratings yet
- Procurement Management Ch12Document43 pagesProcurement Management Ch12AsratNo ratings yet
- EQ EQ EQ EQ A B C: Roof Framing PlanDocument2 pagesEQ EQ EQ EQ A B C: Roof Framing PlanManojNo ratings yet
- Procurement Management: Weatherization Assistance ProgramDocument49 pagesProcurement Management: Weatherization Assistance ProgramManojNo ratings yet
- CSR FR HarjotoDocument36 pagesCSR FR HarjotoManojNo ratings yet
- Managing CSR Issues in The Supply ChainDocument40 pagesManaging CSR Issues in The Supply ChainManojNo ratings yet
- CSR & Corporate FraudDocument18 pagesCSR & Corporate FraudManojNo ratings yet
- Stage 1 Preconstruction Design Contract DocumentsDocument52 pagesStage 1 Preconstruction Design Contract DocumentsnilminaNo ratings yet
- Managing CSR Issues in The Supply ChainDocument40 pagesManaging CSR Issues in The Supply ChainManojNo ratings yet
- CSR FR HarjotoDocument36 pagesCSR FR HarjotoManojNo ratings yet
- Apply teacher short leaveDocument1 pageApply teacher short leaveJean Claudine MandayNo ratings yet
- Types of Solder FluxDocument6 pagesTypes of Solder Fluxpeter paulNo ratings yet
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- VECTOR CONTROL METHODSDocument4 pagesVECTOR CONTROL METHODSmirabelle LovethNo ratings yet
- Unit 4 CommunicationDocument3 pagesUnit 4 Communicationsutarmisaja15No ratings yet
- Five Feet Apart ReviewDocument7 pagesFive Feet Apart ReviewBianca HequilanNo ratings yet
- 2020 Corportate Sustainability ReportDocument22 pages2020 Corportate Sustainability ReportMohamed KannouNo ratings yet
- Health Information Technology-HISMLSDocument1 pageHealth Information Technology-HISMLSJanela Escalante TaboraNo ratings yet
- Synthesis 3 Jay VillasotoDocument6 pagesSynthesis 3 Jay VillasotoJay VillasotoNo ratings yet
- Mercury in The MistDocument2 pagesMercury in The MistAnand BhagwaniNo ratings yet
- Managing STEM AthletesDocument13 pagesManaging STEM Athletesanon_629662799No ratings yet
- Melidiosis FDocument24 pagesMelidiosis FVyramuthu AtputhanNo ratings yet
- CIS ParentDocument2 pagesCIS ParentAbegail (Abby) MirandaNo ratings yet
- Veteran Resource Guide For Congressional District 9Document27 pagesVeteran Resource Guide For Congressional District 9RepSinemaNo ratings yet
- Giraffe and Panda Warmer TRM M1128921 Rev PDocument230 pagesGiraffe and Panda Warmer TRM M1128921 Rev PRonnelSerranoNo ratings yet
- ICICI Bank Mortgage - HS360 Product FinalDocument29 pagesICICI Bank Mortgage - HS360 Product FinalRishu GiriNo ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Guide To Patient Support and Regional Cancer ServicesDocument76 pagesGuide To Patient Support and Regional Cancer Servicesgiovanna2004No ratings yet
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
- Empowering Women Key to Ending PovertyDocument25 pagesEmpowering Women Key to Ending PovertydassmbaNo ratings yet
- ResistanceDocument8 pagesResistanceAndi Soraya WalyddainiNo ratings yet
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- Child Abuse Research JournalDocument9 pagesChild Abuse Research JournaladrianekattnerNo ratings yet