You might also like
- The Code Stroke Handbook: Approach to the Acute Stroke PatientFrom EverandThe Code Stroke Handbook: Approach to the Acute Stroke PatientNo ratings yet
- Cerebrovascular Accident (CVA) "Stroke": Ma. Tosca Cybil A. Torres, RN, MANDocument53 pagesCerebrovascular Accident (CVA) "Stroke": Ma. Tosca Cybil A. Torres, RN, MANMa Tosca Cybil TorresNo ratings yet
- Idiopathic Intracranial Hypertension Explained: A Guide for Patients and FamiliesFrom EverandIdiopathic Intracranial Hypertension Explained: A Guide for Patients and FamiliesNo ratings yet
- Critical Care in NeurologyDocument65 pagesCritical Care in NeurologydrbhawnavermaNo ratings yet
- Vestibular Function Evaluation & DiagnosisDocument98 pagesVestibular Function Evaluation & DiagnosisЭ.ТөгөлдөрNo ratings yet
- Nanda NCP BasedDocument14 pagesNanda NCP Baseddeliejoyce100% (1)
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDocument352 pagesAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNo ratings yet
- Alisha Allana - Clinical Cases For The FRCA - Key Topics Mapped To The RCoA Curriculum-CRC Press (2022)Document253 pagesAlisha Allana - Clinical Cases For The FRCA - Key Topics Mapped To The RCoA Curriculum-CRC Press (2022)Matthew Marion100% (2)
- Head InjuryDocument50 pagesHead InjuryThiagarajah RaviNo ratings yet
- Seminar ON Seizure: Presented To Presented byDocument35 pagesSeminar ON Seizure: Presented To Presented byShitaljit IromNo ratings yet
- Subarachnoid HemorrhageDocument16 pagesSubarachnoid HemorrhageErika NaingNo ratings yet
- Common Medical Emergencies: Jude D. Positos, RNDocument27 pagesCommon Medical Emergencies: Jude D. Positos, RNNenen PositosNo ratings yet
- Pub Family Practice Examination and Board ReviewDocument937 pagesPub Family Practice Examination and Board ReviewMohammad PharaonNo ratings yet
- The Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Document66 pagesThe Role of EEG in The Diagnosis and Classification of The Epilepsy Syndromes (Part 1)Rosmery VillaNo ratings yet
- Neurological AssessmentDocument20 pagesNeurological Assessmentdhanya jayan100% (1)
- Lesson Plan On SeizureDocument6 pagesLesson Plan On SeizureJeya vanithaNo ratings yet
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- Inibuilds A310 MSFS ManualDocument79 pagesInibuilds A310 MSFS ManualShrinivasan TNo ratings yet
- Case PresentationDocument34 pagesCase PresentationAdelle Fortunato100% (1)
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Management OF Head Injury: DR Echebiri, PDocument26 pagesManagement OF Head Injury: DR Echebiri, PLuther ThengNo ratings yet
- CBT Neurosurgery - TutorDocument24 pagesCBT Neurosurgery - Tutoramoody95No ratings yet
- Case PresentationDocument41 pagesCase PresentationAhmad NawazNo ratings yet
- Third Problem "Shake Rattle & Roll: Group 09 Tuesday, 8 Oct 2019Document51 pagesThird Problem "Shake Rattle & Roll: Group 09 Tuesday, 8 Oct 2019waraney palitNo ratings yet
- Mon 11-30 Neuroimaging Pearls For The Primary Care Provider - 0Document25 pagesMon 11-30 Neuroimaging Pearls For The Primary Care Provider - 0regarskidNo ratings yet
- A Case Study Presentation On Subarachnoid Hemorrhage: Presented byDocument78 pagesA Case Study Presentation On Subarachnoid Hemorrhage: Presented byNina100% (1)
- Introduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersDocument142 pagesIntroduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersomarNo ratings yet
- Neurology Case Protocol DATORDocument4 pagesNeurology Case Protocol DATORDon Peter DatorNo ratings yet
- Demyelinating DiseaseDocument42 pagesDemyelinating Diseasemirabel IvanaliNo ratings yet
- EMRC Headache Slides 2upDocument33 pagesEMRC Headache Slides 2upMohammed AlrashedNo ratings yet
- Chapter 2 Intro To Brain ImagingDocument49 pagesChapter 2 Intro To Brain ImagingJellie MendozaNo ratings yet
- Neurology Case Protocol DATORDocument4 pagesNeurology Case Protocol DATORDon Peter DatorNo ratings yet
- Neuro Case PresentationsDocument25 pagesNeuro Case PresentationsTSunamiNo ratings yet
- Neuroscience Syllabus Fall 2013Document5 pagesNeuroscience Syllabus Fall 2013Anonymous t5TDwd100% (1)
- Terson Syndrome: Don't Let It Go Unrecognized: Ophthalmic PearlsDocument2 pagesTerson Syndrome: Don't Let It Go Unrecognized: Ophthalmic PearlsSherley CruzNo ratings yet
- EpilepsyDocument41 pagesEpilepsyaboubakarylwabukobaNo ratings yet
- Fainting and Blacking Out (Near-Syncope and Syncope) .: - o o o o o o oDocument3 pagesFainting and Blacking Out (Near-Syncope and Syncope) .: - o o o o o o oLILY MAINNo ratings yet
- Aneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyDocument100 pagesAneurysmal Subarachnoid Hemorrhage Nursing Self-Paced Case StudyAndi rahma AnugrahNo ratings yet
- Epidural Haematoma: DR - Karan R RawatDocument65 pagesEpidural Haematoma: DR - Karan R RawatSitha ChristineNo ratings yet
- Cva Case Ms 4th Rotation Final FileDocument65 pagesCva Case Ms 4th Rotation Final FileNursing DepartmentNo ratings yet
- SchizophreniaDocument33 pagesSchizophreniaGgabri ELaNo ratings yet
- ENLS Sub-Arachnoid Hemorrhage ProtocolDocument22 pagesENLS Sub-Arachnoid Hemorrhage ProtocolFransiskus MikaelNo ratings yet
- Laporan Tutorial Skenario 3: Sabrina Fazriesa 1418011194Document28 pagesLaporan Tutorial Skenario 3: Sabrina Fazriesa 1418011194Sabrina FazriesaNo ratings yet
- Nursing Care Plan Format X1Document3 pagesNursing Care Plan Format X1Ramiel ChristopherNo ratings yet
- Patient Behaviour Case Based Presentation: DeliriumDocument112 pagesPatient Behaviour Case Based Presentation: Deliriumb BNo ratings yet
- PocketCard Assessment and Management of Stroke July 2020Document12 pagesPocketCard Assessment and Management of Stroke July 2020chellczyNo ratings yet
- 9 JosephsonDocument19 pages9 JosephsonTizazu BayihNo ratings yet
- Park Inso N'S Dise ASEDocument132 pagesPark Inso N'S Dise ASEGrace Dela Rosa MelecioNo ratings yet
- Chapter 5Document9 pagesChapter 5Aristya EkaputraNo ratings yet
- All Previous Essay Surgery 2Document162 pagesAll Previous Essay Surgery 2DR/ AL-saifiNo ratings yet
- 2019 Enls For ApacvsnnnnnnDocument46 pages2019 Enls For ApacvsnnnnnnAhmed ElshewiNo ratings yet
- Anti Nmdar EncephalitisDocument2 pagesAnti Nmdar EncephalitisbugogiNo ratings yet
- Identifyingandmanagingacutestroke 150520143046 Lva1 App6892Document62 pagesIdentifyingandmanagingacutestroke 150520143046 Lva1 App6892Raghu NadhNo ratings yet
- ASN 2016 UPDATE Flash DriveDocument119 pagesASN 2016 UPDATE Flash DrivethisarNo ratings yet
- StrokeDocument6 pagesStrokebrendavenegasNo ratings yet
- Update: Management of Head InjuriesDocument38 pagesUpdate: Management of Head InjuriesRoby Aditya SuryaNo ratings yet
- Update: Management of Head InjuriesDocument38 pagesUpdate: Management of Head InjuriesWilly OematanNo ratings yet
- Brain InjuryDocument35 pagesBrain InjuryAkhil Adhithyan RamNo ratings yet
- Approach To Body Weakness - StrokeDocument13 pagesApproach To Body Weakness - StrokeHynne Jhea EchavezNo ratings yet
- Practice Station Headache HXDocument7 pagesPractice Station Headache HXWenbin GuoNo ratings yet
- Hemorragia Intracraneal EspontaneaDocument7 pagesHemorragia Intracraneal Espontaneajosue leonardo RuizNo ratings yet
- Trigeminal NeuralgiaDocument72 pagesTrigeminal NeuralgiaCocoMathewNo ratings yet
- CP On CVADocument103 pagesCP On CVAanupama vargheseNo ratings yet
- Invasive Neuromonitoring TechniqueDocument20 pagesInvasive Neuromonitoring TechniqueReza ManefoNo ratings yet
- Acute Ischemic StrokeDocument9 pagesAcute Ischemic Strokepuskesmas tarikNo ratings yet
- Patient Management Problem Preferred Responses.27Document12 pagesPatient Management Problem Preferred Responses.27mhd.mamdohNo ratings yet
- Jurnal International AbortusDocument9 pagesJurnal International AbortusarvinaNo ratings yet
- Pre Anesthesia Assessment and PreparationDocument8 pagesPre Anesthesia Assessment and PreparationNoviantiNo ratings yet
- ABIM Laboratory Test Reference Ranges January 2020Document12 pagesABIM Laboratory Test Reference Ranges January 2020jaumeNo ratings yet
- Jurding 3 Combined Treatment With Chondroitin Sulfate and Glucosamine Sulfate Shows No Superiority Over Placebofor Reduction of JDocument9 pagesJurding 3 Combined Treatment With Chondroitin Sulfate and Glucosamine Sulfate Shows No Superiority Over Placebofor Reduction of JCeryle EriadyNo ratings yet
- Ppok Eksaserbasi Dr. Hadisono, SP.P Fakultas Kedokteran Universitas TarumanagaraDocument13 pagesPpok Eksaserbasi Dr. Hadisono, SP.P Fakultas Kedokteran Universitas TarumanagaraCeryle EriadyNo ratings yet
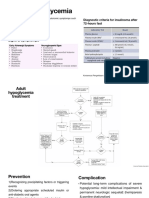
- Severe Hypoglycemia: Diagnostic Criteria For Insulinoma After 72-Hours FastDocument3 pagesSevere Hypoglycemia: Diagnostic Criteria For Insulinoma After 72-Hours FastCeryle EriadyNo ratings yet
- Heavy Metal CerDocument4 pagesHeavy Metal CerCeryle EriadyNo ratings yet
- Heavy Metal CerDocument4 pagesHeavy Metal CerCeryle EriadyNo ratings yet
- Length-For-Age GIRLS: Birth To 6 Months (Percentiles)Document15 pagesLength-For-Age GIRLS: Birth To 6 Months (Percentiles)Ceryle EriadyNo ratings yet
- Chts Girls ZDocument15 pagesChts Girls ZCeryle EriadyNo ratings yet
- ABIM Laboratory Test Reference Ranges January 2020Document12 pagesABIM Laboratory Test Reference Ranges January 2020jaumeNo ratings yet
- Tugas Dr. Saelan - Kelompok 7 - PJJ Jwa Periode 26 April-1 Mei 2021Document83 pagesTugas Dr. Saelan - Kelompok 7 - PJJ Jwa Periode 26 April-1 Mei 2021michael palitNo ratings yet
- Chole CystitisDocument13 pagesChole CystitisColdicedNo ratings yet
- Lapkas ObgynDocument4 pagesLapkas ObgynCeryle EriadyNo ratings yet
- The Child With Neurologic Disorder: Group Iv - Bsn2BDocument100 pagesThe Child With Neurologic Disorder: Group Iv - Bsn2BNics FranciscoNo ratings yet
- Sunflower Syndrome GuideDocument19 pagesSunflower Syndrome GuidetkarkleNo ratings yet
- Epilepsia - 2005 - Knudsen - Febrile Seizures Treatment and PrognosisDocument8 pagesEpilepsia - 2005 - Knudsen - Febrile Seizures Treatment and PrognosisJanina MaligayaNo ratings yet
- People v. DecinaDocument10 pagesPeople v. Decinacansuzorman8No ratings yet
- Breath-Holding Spells (Article) Author Seattle Children'sDocument2 pagesBreath-Holding Spells (Article) Author Seattle Children'sNicholas DurityNo ratings yet
- Guitar Hero III - Manual - WII PDFDocument11 pagesGuitar Hero III - Manual - WII PDFJames WilliamsNo ratings yet
- Module 4 - Approach To The Comatose PatientDocument35 pagesModule 4 - Approach To The Comatose PatientRick RanitNo ratings yet
- Case Study SBI242Document6 pagesCase Study SBI242Sky KaurNo ratings yet
- Seizure Management in Dogs: Consultant On CallDocument5 pagesSeizure Management in Dogs: Consultant On CallGissele ParaisoNo ratings yet
- Thyroid Data Pediatric PatientDocument31 pagesThyroid Data Pediatric Patientبشير حيدرNo ratings yet
- NSwitch ImportantInformation UKVDocument5 pagesNSwitch ImportantInformation UKVabc defNo ratings yet
- Antiepileptic Medicines Shanbhag ShenoyDocument9 pagesAntiepileptic Medicines Shanbhag Shenoyshaziashaziashazia2001No ratings yet
- Relocation of NGCP Transmission PostDocument14 pagesRelocation of NGCP Transmission PostHd SecretariatNo ratings yet
- Prepared by Prof. Dr. Soliman TahoonDocument15 pagesPrepared by Prof. Dr. Soliman TahoonEgyptian BookstoreNo ratings yet
- Drug Utilization Study of Antiepileptic Drugs In.21Document6 pagesDrug Utilization Study of Antiepileptic Drugs In.21Ramo EdumNo ratings yet
- Ravizza Et Al. 2011Document8 pagesRavizza Et Al. 2011JD SánchezNo ratings yet
- Molecules 26 04535 v2Document26 pagesMolecules 26 04535 v2George NeaguNo ratings yet
- ALOC Can Be Caused by A Head Injury, Medicines, Alcohol or Drugs, Dehydration, or Some Diseases, Such As DiabetesDocument9 pagesALOC Can Be Caused by A Head Injury, Medicines, Alcohol or Drugs, Dehydration, or Some Diseases, Such As DiabetesDinarkram Rabreca EculNo ratings yet
- CNS Seizures in ChildhoodDocument42 pagesCNS Seizures in ChildhoodDr.P.NatarajanNo ratings yet
- HALO Combat Evolved Anniversary ManualDocument7 pagesHALO Combat Evolved Anniversary ManualJohnny GatNo ratings yet
- Misra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiaDocument10 pagesMisra U, Kalita J Dan Dubey D. A Study of Super Refractory Status Epilepticus From IndiasitialimahNo ratings yet
- NCM 106 (PHARMA) - Lec 19 To 28Document18 pagesNCM 106 (PHARMA) - Lec 19 To 28Aine Jermaine GatchalianNo ratings yet
- Neurological Disorders Key NotesDocument31 pagesNeurological Disorders Key NotesHannah aswiniNo ratings yet