You might also like
- Laboratory Investigations in Uveitis: Dr. Sriniwas Atal 1 Year Resident OphthalmologyDocument39 pagesLaboratory Investigations in Uveitis: Dr. Sriniwas Atal 1 Year Resident OphthalmologySriniwasNo ratings yet
- Personality and Arousal: A Psychophysiological Study of Psychiatric DisorderFrom EverandPersonality and Arousal: A Psychophysiological Study of Psychiatric DisorderNo ratings yet
- Ostrosky Neuropsi Attención MemoryDocument17 pagesOstrosky Neuropsi Attención MemoryMax HosteelNo ratings yet
- Brain Anatomy, Anatomy of The Human Brain - Mayfield Brain & Spine Cincinnati, Ohio 2 PDFDocument20 pagesBrain Anatomy, Anatomy of The Human Brain - Mayfield Brain & Spine Cincinnati, Ohio 2 PDFRitika KishoreNo ratings yet
- Diagnostic Considerations in Uveitis: Anatomy, Signs, Symptoms and Differential DiagnosisDocument43 pagesDiagnostic Considerations in Uveitis: Anatomy, Signs, Symptoms and Differential DiagnosisevaNo ratings yet
- The Effect of Core Stability Training On Dynamic Balance and Smash Stroke Performance in Badminton PlayersDocument9 pagesThe Effect of Core Stability Training On Dynamic Balance and Smash Stroke Performance in Badminton Playersanon_269306840No ratings yet
- Psychotherapy and MentoringDocument38 pagesPsychotherapy and MentoringImon PaulNo ratings yet
- NeuropsychologyDocument7 pagesNeuropsychologyAbby Orioque IINo ratings yet
- Mini-Mental State Exam: Right / Wrong? - 30 Questions For 30 PointsDocument3 pagesMini-Mental State Exam: Right / Wrong? - 30 Questions For 30 Pointsmediana fitriNo ratings yet
- Handouts YBOC Symptom ChecklistDocument2 pagesHandouts YBOC Symptom ChecklistJoem cNo ratings yet
- The Role of in The OF: CAM TreatmentDocument47 pagesThe Role of in The OF: CAM TreatmenterinahuntNo ratings yet
- AMNESIC DISORDERS OVERVIEWDocument55 pagesAMNESIC DISORDERS OVERVIEWdrkadiyala2No ratings yet
- NBSE Evidence-Based Review Test Summary TablesDocument82 pagesNBSE Evidence-Based Review Test Summary TablesIcaroNo ratings yet
- Cernyetal.2022 SluggishCognitiveTempo JADDocument12 pagesCernyetal.2022 SluggishCognitiveTempo JADmahsaNo ratings yet
- Estimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciaDocument14 pagesEstimation of Premorbid Intelligence in Spanish People With The Word Accentuation Test and Its Application To The Diagnosis of DemenciathebeholderNo ratings yet
- Brain Anatomy, Anatomy of The Human BrainDocument12 pagesBrain Anatomy, Anatomy of The Human BrainElmir ƏzimovNo ratings yet
- 4960 4843 1 PB PDFDocument21 pages4960 4843 1 PB PDFSartini Roma Dame NainggolanNo ratings yet
- Validation of Moca Test in Vietnamese Language For Cognitive Impairment ScreeningDocument17 pagesValidation of Moca Test in Vietnamese Language For Cognitive Impairment ScreeningMolly DangNo ratings yet
- Halstead Reitan & Luria Nebraska Battery: by Prasad Jadhav Ma IiDocument33 pagesHalstead Reitan & Luria Nebraska Battery: by Prasad Jadhav Ma IiMarcella Mariska AryonoNo ratings yet
- Boston Qualitative Scoring System for Rey-Osterrieth Complex Figure Effective for Detecting Cognitive Impairment in Parkinson's DiseaseDocument9 pagesBoston Qualitative Scoring System for Rey-Osterrieth Complex Figure Effective for Detecting Cognitive Impairment in Parkinson's DiseaseJuanNo ratings yet
- ( (#Ve?@ (2 ( (#Ve?@ (G ( (#Ve?@ (M (R6 (,cbwxcd@yz (KG54GN ( (V/6L (Document1 page( (#Ve?@ (2 ( (#Ve?@ (G ( (#Ve?@ (M (R6 (,cbwxcd@yz (KG54GN ( (V/6L (Ramiro ReckziegelNo ratings yet
- EXIT25 Executive InterviewDocument10 pagesEXIT25 Executive InterviewZeeshan Ali100% (1)
- Psychometrics Lecture 2Document58 pagesPsychometrics Lecture 2Mac SensNo ratings yet
- Management For Multiple HandicapDocument57 pagesManagement For Multiple HandicapMSc Audio BNo ratings yet
- Cerad Total ScoreDocument6 pagesCerad Total ScorecoconitaNo ratings yet
- Mindfulness-Based Stress Reduction (MBSR) : MBSR Instructor Peggy ChangDocument26 pagesMindfulness-Based Stress Reduction (MBSR) : MBSR Instructor Peggy ChangstevechrNo ratings yet
- Lifespan Development - Relationships Through The Lifespan - Julia Diorio and Nick Rause - 2Document18 pagesLifespan Development - Relationships Through The Lifespan - Julia Diorio and Nick Rause - 2api-533586515No ratings yet
- NPT Report DataDocument3 pagesNPT Report Datafiend007No ratings yet
- Final ThesisDocument120 pagesFinal ThesisSingh SoniyaNo ratings yet
- Brain Injury and Epilepsy: What Is An Epileptic Seizure?Document4 pagesBrain Injury and Epilepsy: What Is An Epileptic Seizure?kaninerNo ratings yet
- The "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderDocument3 pagesThe "when" and "where" of α-synucleinopathies: Insights from REM sleep behavior disorderSandsackNo ratings yet
- 6-Rourke, B.P. (2005)Document5 pages6-Rourke, B.P. (2005)iilolii.ch3495No ratings yet
- 25021Document18 pages25021Reena Singh SheoranNo ratings yet
- 16PF BibDocument10 pages16PF BibdocagunsNo ratings yet
- Patient-Rated Anxiety Scale: Quickly Identifies Anxiety Symptom SeverityDocument2 pagesPatient-Rated Anxiety Scale: Quickly Identifies Anxiety Symptom SeveritySisy AnandaNo ratings yet
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 pagesSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimNo ratings yet
- PSQIDocument2 pagesPSQIAdrian HartantoNo ratings yet
- Indications For NeuropsychologicalDocument5 pagesIndications For NeuropsychologicalIcaroNo ratings yet
- Intelligence and Emotional Disorders - PAID - 2015 PDFDocument4 pagesIntelligence and Emotional Disorders - PAID - 2015 PDFOmar Azaña Velez100% (1)
- An Update On The Comorbidity of ADHD and ASDDocument16 pagesAn Update On The Comorbidity of ADHD and ASDCristina SolerNo ratings yet
- Dados Normativos BICAMS para Esclerose Múltipla No BrasilDocument11 pagesDados Normativos BICAMS para Esclerose Múltipla No BrasilCarina TellaroliNo ratings yet
- Dementia Symptoms ChecklistDocument16 pagesDementia Symptoms ChecklistAnand Prakash SinghNo ratings yet
- Memoryarticles: The Three Memory Storage SystemsDocument17 pagesMemoryarticles: The Three Memory Storage SystemsZein YusufNo ratings yet
- STROOP InstructionsDocument8 pagesSTROOP InstructionsScribdTranslations100% (1)
- The MMSEDocument4 pagesThe MMSESiti Zubaidah HussinNo ratings yet
- Depression Among Medical (MBBS) Students of India: Meta AnalysisDocument8 pagesDepression Among Medical (MBBS) Students of India: Meta AnalysisAnonymous x8fY69CrnNo ratings yet
- Assessing Child Behavior with Focal AssessmentDocument18 pagesAssessing Child Behavior with Focal AssessmentFaten SalahNo ratings yet
- Rorschach Profile of Indian Adults: July 2010Document17 pagesRorschach Profile of Indian Adults: July 2010Suresh Lukose100% (1)
- Suppl55 PDFDocument310 pagesSuppl55 PDFUbaidillah Romadlon AlfairuziNo ratings yet
- Visual Agnosia - FarahDocument207 pagesVisual Agnosia - Farahrocolmar100% (1)
- Negative Symptoms EQZ Lancet ReviewDocument14 pagesNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezNo ratings yet
- A Manual For Objective TAT ScoringDocument40 pagesA Manual For Objective TAT ScoringJaveriaNo ratings yet
- Watson (1988) - Development and Validation of Brief Measures of Positive and Negative Affect The PANAS ScalesDocument8 pagesWatson (1988) - Development and Validation of Brief Measures of Positive and Negative Affect The PANAS ScalesElwood BluesNo ratings yet
- Long Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreDocument55 pagesLong Term Pharmacotherapy For Alcohol Dependence: Centre of Addiction Medicine NIMHANS, BangaloreGirish NagarNo ratings yet
- Cognitive DisordersDocument3 pagesCognitive DisordersKayze UbaldoNo ratings yet
- Sacs Sub ScaleDocument2 pagesSacs Sub Scaleastridich100% (1)
- Parietal Lobe SyndromeDocument14 pagesParietal Lobe Syndromefita9candraNo ratings yet
- Chapter 5 Powerpoint With Extra SlidesDocument111 pagesChapter 5 Powerpoint With Extra Slidesmonster40lbsNo ratings yet
- BKT NotesDocument6 pagesBKT NotesPallavi ChopraNo ratings yet
- Nuisance CandidateDocument5 pagesNuisance CandidateMalen AvanceñaNo ratings yet
- Jane Austen's Literary StyleDocument4 pagesJane Austen's Literary StyleGulfam RashidNo ratings yet
- International Organizations and RelationsDocument3 pagesInternational Organizations and RelationsPachie MoloNo ratings yet
- Test Bank For Oral Pathology 7th Edition by RegeziDocument11 pagesTest Bank For Oral Pathology 7th Edition by RegeziSteve Isola100% (23)
- En Subject C08Document13 pagesEn Subject C08jmolfigueiraNo ratings yet
- Bible Walk Through - Old TestamentDocument211 pagesBible Walk Through - Old TestamentWei Wang100% (2)
- Indigenous Peoples SyllabusDocument9 pagesIndigenous Peoples Syllabusapi-263787560No ratings yet
- Henry D. Solatorio Jr. NCM 105: Promote Good Blood Sugar (Glucose) LevelsDocument2 pagesHenry D. Solatorio Jr. NCM 105: Promote Good Blood Sugar (Glucose) LevelsCristoper BodionganNo ratings yet
- PNB's Financial Inclusion Initiatives and TechnologiesDocument18 pagesPNB's Financial Inclusion Initiatives and TechnologiesShreya DubeyNo ratings yet
- PETDocument4 pagesPETMaria Dolores Barrionuevo AlvarezNo ratings yet
- Introduction To Robotics: Why Build Robots?Document10 pagesIntroduction To Robotics: Why Build Robots?api-115728880No ratings yet
- 285519-35126-30-case-studyDocument12 pages285519-35126-30-case-studyapi-737834018No ratings yet
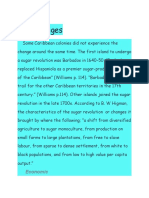
- Effects of The Sugar RevolutionDocument9 pagesEffects of The Sugar RevolutionSusan BarriotNo ratings yet
- Syllabus Changes: March 2021 Version 1Document20 pagesSyllabus Changes: March 2021 Version 1Azul IrlaundeNo ratings yet
- Group No 5 - Ultratech - Jaypee 20th Sep-1Document23 pagesGroup No 5 - Ultratech - Jaypee 20th Sep-1Snehal100% (1)
- Hydraulic Caliper Service Manual MM0266Document27 pagesHydraulic Caliper Service Manual MM0266LUKASNo ratings yet
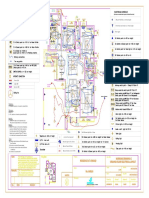
- Varun Valanjeri Electrical Layout-3Document1 pageVarun Valanjeri Electrical Layout-3ANOOP R NAIRNo ratings yet
- IEC 61850 Configuration of A Phoenix Contact IED: User ManualDocument68 pagesIEC 61850 Configuration of A Phoenix Contact IED: User ManualHarold PuinNo ratings yet
- 1.1.5.a Elisa-3Document3 pages1.1.5.a Elisa-3Zainab DioufNo ratings yet
- Current Openings: The Sirpur Paper Mills LTDDocument3 pagesCurrent Openings: The Sirpur Paper Mills LTDMano VardhanNo ratings yet
- Cad MCQ Unit 5Document3 pagesCad MCQ Unit 5ddeepak123No ratings yet
- Lesson 19 - Preparation of Capital Statement and Balance SheetDocument6 pagesLesson 19 - Preparation of Capital Statement and Balance SheetMayeng MonayNo ratings yet
- Chapter 3 The Life of Jose Rizal PDFDocument11 pagesChapter 3 The Life of Jose Rizal PDFMelanie CaplayaNo ratings yet
- Cing - Common Interface For NMR Structure Generation: Results 1 - 10 of 978Document3 pagesCing - Common Interface For NMR Structure Generation: Results 1 - 10 of 978Judap FlocNo ratings yet
- How To Comp For A Vocalist - Singer - The Jazz Piano SiteDocument5 pagesHow To Comp For A Vocalist - Singer - The Jazz Piano SiteMbolafab RbjNo ratings yet
- Oracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentDocument4 pagesOracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentRamón MedinaNo ratings yet
- Mil STD 1365bDocument49 pagesMil STD 1365bprakki123No ratings yet
- Advanced Accounting PDFDocument14 pagesAdvanced Accounting PDFYvette Pauline JovenNo ratings yet
- MS For SprinklerDocument78 pagesMS For Sprinklerkarthy ganesanNo ratings yet
- En 10025 PDFDocument35 pagesEn 10025 PDFAbdelali88% (8)