You might also like
- Nefrologia 30 Dias Electrolitos3Document31 pagesNefrologia 30 Dias Electrolitos3JUAN ANDRES GUARDIAS GARZONNo ratings yet
- Adrenal Gland Physiology (DRDocument77 pagesAdrenal Gland Physiology (DRapi-3769252100% (4)
- 1 Metabolic Response To Injury PDFDocument50 pages1 Metabolic Response To Injury PDFyayayanizaNo ratings yet
- Chapter 21 - Responding To The Cellular EnvironmentDocument29 pagesChapter 21 - Responding To The Cellular EnvironmentRebecca Long HeiseNo ratings yet
- 003Document358 pages003Gordana UzelacNo ratings yet
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Hiper K CCM2008Document6 pagesHiper K CCM2008Carol ArraisNo ratings yet
- 1.neuro Endocrne Response To SurgeryDocument42 pages1.neuro Endocrne Response To SurgeryEngidawork MaruNo ratings yet
- Introduction to Physiology: Homeostasis and Feedback MechanismsDocument58 pagesIntroduction to Physiology: Homeostasis and Feedback MechanismsChiedza MutigwaNo ratings yet
- 1 Metabolic Response To InjuryDocument38 pages1 Metabolic Response To InjuryyayayanizaNo ratings yet
- Shock: Clinical ManifestationsDocument3 pagesShock: Clinical ManifestationsJean ReyesNo ratings yet
- AdrenocorticosteroidsDocument64 pagesAdrenocorticosteroidsGeraldine Marie SalvoNo ratings yet
- Management of Potassium Disorders 17706 ArticleDocument4 pagesManagement of Potassium Disorders 17706 ArticlealeNo ratings yet
- General Physiology PDFDocument11 pagesGeneral Physiology PDFmedpgnotes100% (4)
- Metabolic response to injuryDocument5 pagesMetabolic response to injuryZllison Mae Teodoro Mangabat100% (1)
- Engle Hart 2006Document6 pagesEngle Hart 2006pinandhitaNo ratings yet
- Hyperglycemia Syndromes: Diabetic Ketoacidosis Ketoacidosis-Hypersomolar ComaDocument35 pagesHyperglycemia Syndromes: Diabetic Ketoacidosis Ketoacidosis-Hypersomolar ComaPriyanka ChampanerkarNo ratings yet
- Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar SyndromeDocument59 pagesDiabetic Ketoacidosis and Hyperglycemic Hyperosmolar Syndromenatalieshirley100% (1)
- Weakness Following Diarrhea: 1/4: 1. What Can Be The Cause of Her Condition?Document4 pagesWeakness Following Diarrhea: 1/4: 1. What Can Be The Cause of Her Condition?ZauzaNo ratings yet
- Fluid and ElectrolytesDocument23 pagesFluid and ElectrolytesNanaNo ratings yet
- I.V. FluidsDocument33 pagesI.V. FluidsVineel Bezawada100% (1)
- Physiology of The Adrenal Gland: DR Nyein Nyein Wai Associate ProfessorDocument42 pagesPhysiology of The Adrenal Gland: DR Nyein Nyein Wai Associate ProfessorAzizan HannyNo ratings yet
- CorticosteroidsDocument42 pagesCorticosteroidsejiNo ratings yet
- Systemic Response To InjuryDocument7 pagesSystemic Response To Injuryjc_sibal13No ratings yet
- Metabolic Stress PDFDocument30 pagesMetabolic Stress PDFNurul Latifa MuhammadNo ratings yet
- CorticosteroidsDocument63 pagesCorticosteroidsRiddhi Jain100% (2)
- Hiperkalemia en Paceintes Con HemodialisisDocument12 pagesHiperkalemia en Paceintes Con HemodialisisperezlimacarlosandresNo ratings yet
- Pharmacodynamic Pharmacokinetic of CorticosteroidDocument34 pagesPharmacodynamic Pharmacokinetic of CorticosteroidIvaNo ratings yet
- Review of LaboratoryDocument48 pagesReview of LaboratoryIkhar RidhoNo ratings yet
- Physiology DR - KKDocument259 pagesPhysiology DR - KKHARIHARAN VNo ratings yet
- PERFUSION monitoring-SYSTEMIC-ghalebDocument49 pagesPERFUSION monitoring-SYSTEMIC-ghalebGHALEB A. AlmekhlafiNo ratings yet
- Nutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Document108 pagesNutritional Management On Kidney Disease: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK 2018Rahmawati HamudiNo ratings yet
- Sign up to receive ATOTW weeklyDocument9 pagesSign up to receive ATOTW weeklyAbhishek LonikarNo ratings yet
- Review of Laboratory and Diagnostic TestsDocument41 pagesReview of Laboratory and Diagnostic TestsPutri Anggraini Rusanti100% (1)
- Hyponatremia in DCLDDocument27 pagesHyponatremia in DCLDGowtham KrishnaNo ratings yet
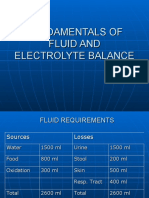
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistNo ratings yet
- Adrenal Control Within The Body: Presented byDocument20 pagesAdrenal Control Within The Body: Presented byhumnaNo ratings yet
- 003 - DM - Acute ComplicationsDocument17 pages003 - DM - Acute ComplicationsLucas Victor AlmeidaNo ratings yet
- Derangements of Potassium - Emergency Medicine 2014Document19 pagesDerangements of Potassium - Emergency Medicine 2014Michael AmarilloNo ratings yet
- Quang Bui - Rifaximin and Hepatic Encephalopathy FINALDocument32 pagesQuang Bui - Rifaximin and Hepatic Encephalopathy FINALtomoe hotaru100% (1)
- Enzymology Definitions and TerminologyDocument23 pagesEnzymology Definitions and TerminologyCalvin Yeow-kuan ChongNo ratings yet
- Metabolic Response To TraumaDocument40 pagesMetabolic Response To TraumaEdwin OkonNo ratings yet
- Diabetic KetoacidosisDocument41 pagesDiabetic KetoacidosisdenekeNo ratings yet
- Distribution of This Potassium Between The Extracellular and Intracellular FluidDocument9 pagesDistribution of This Potassium Between The Extracellular and Intracellular FluidLovelle LopezNo ratings yet
- Journal Club: Paolo Dametto January 2013Document42 pagesJournal Club: Paolo Dametto January 2013Олег ЕвсюковNo ratings yet
- Circadian Rhythms and Diabetes: How Disrupted Clocks Can Lead to DiseaseDocument2 pagesCircadian Rhythms and Diabetes: How Disrupted Clocks Can Lead to DiseaseDwi afrianti Rahma putriNo ratings yet
- Body Composition & Homeostasis 2022Document34 pagesBody Composition & Homeostasis 2022Charmaine LucNo ratings yet
- Bioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Document44 pagesBioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Andrea ModestieNo ratings yet
- Clinically Important EnzymesDocument29 pagesClinically Important Enzymesonnumilla49No ratings yet
- General Principles of HomeostasisDocument33 pagesGeneral Principles of HomeostasisSatriya Wibawa100% (1)
- 2.physiology Emrcs2016Document195 pages2.physiology Emrcs2016Farah FarahNo ratings yet
- 1.7 Fluids PDFDocument6 pages1.7 Fluids PDFusamaNo ratings yet
- Diabetic Ketoacidosis: Hyperglycemia, Ketosis and AcidosisDocument19 pagesDiabetic Ketoacidosis: Hyperglycemia, Ketosis and AcidosisToNijeToniNo ratings yet
- Lecture 1 - Introduction To Physiology - MD1 2018Document33 pagesLecture 1 - Introduction To Physiology - MD1 2018mus zaharaNo ratings yet
- Corticosteroid Physiology and Principles of Therapy PDFDocument6 pagesCorticosteroid Physiology and Principles of Therapy PDFTriawan AdinataNo ratings yet
- Apoptosis, Brain Protection, Ischemic Preconditioning, Hibernating Bears, and The Western Painted TurtleDocument46 pagesApoptosis, Brain Protection, Ischemic Preconditioning, Hibernating Bears, and The Western Painted TurtleNeurosurgery RmlNo ratings yet
- A14593 Aldehyde Dehydrogenase 2 ALDH2 Glu504Lys.295Document1 pageA14593 Aldehyde Dehydrogenase 2 ALDH2 Glu504Lys.295Iqra RamadaniNo ratings yet
- Corticosteroids Regulation and Clinical UsesDocument36 pagesCorticosteroids Regulation and Clinical UsesAbdur RafayNo ratings yet
- SteroidsDocument25 pagesSteroidsalhusien.abd2000No ratings yet
- Head TraumaDocument3 pagesHead TraumaspiritNo ratings yet
- Cervocal Lateral MassDocument3 pagesCervocal Lateral MassspiritNo ratings yet
- Pedicle Screw Insertion ENNDocument29 pagesPedicle Screw Insertion ENNspiritNo ratings yet
- OPLLDocument3 pagesOPLLspiritNo ratings yet
- Periferal NerveDocument2 pagesPeriferal NervespiritNo ratings yet
- Status EpileptikusDocument5 pagesStatus EpileptikusspiritNo ratings yet
- Imaging - AngiografiDocument10 pagesImaging - AngiografispiritNo ratings yet
- Chap 26 Anatomy Sylvian FissureDocument44 pagesChap 26 Anatomy Sylvian FissurespiritNo ratings yet
- Chap 18 Brain Metastase ENNDocument34 pagesChap 18 Brain Metastase ENNspiritNo ratings yet
- Chap 20 Brainstem TumorDocument34 pagesChap 20 Brainstem TumorspiritNo ratings yet
- ENN Chap 16Document68 pagesENN Chap 16spiritNo ratings yet
- Chap 19 Neurocutaneus SyndromeDocument40 pagesChap 19 Neurocutaneus SyndromespiritNo ratings yet
- As Treatment Options For Shunt Migration To Scrotum: Case Report" by JanuarmanDocument1 pageAs Treatment Options For Shunt Migration To Scrotum: Case Report" by JanuarmanspiritNo ratings yet
- Cover Letter SYSREV ETV VPDocument1 pageCover Letter SYSREV ETV VPspiritNo ratings yet
- Sinonasal Anatomy AA SBY 2017Document48 pagesSinonasal Anatomy AA SBY 2017spiritNo ratings yet
- Nutrisi-Cairan NSDocument30 pagesNutrisi-Cairan NSspiritNo ratings yet
- Dokter Adalah Nurani: Bukan Materi, Jabatan Atau PamrihDocument59 pagesDokter Adalah Nurani: Bukan Materi, Jabatan Atau PamrihspiritNo ratings yet
- Neurosurgical Approach - FinalDocument43 pagesNeurosurgical Approach - Finalspirit100% (2)
- Week 2 - NeuroanatomyDocument29 pagesWeek 2 - NeuroanatomyspiritNo ratings yet
- Sistem Limbik: Moh. Fadli Said, Joni Wahyuhadi Dept - Ot Neurosurgery DR Soetomo Hospital-Med Faculty OfunairDocument13 pagesSistem Limbik: Moh. Fadli Said, Joni Wahyuhadi Dept - Ot Neurosurgery DR Soetomo Hospital-Med Faculty OfunairspiritNo ratings yet
- Brain VentricleDocument40 pagesBrain VentriclespiritNo ratings yet
- Transpetrosal ApproachDocument6 pagesTranspetrosal ApproachspiritNo ratings yet
- Physiology of CSF FixDocument10 pagesPhysiology of CSF FixspiritNo ratings yet
- Background and PathophysiologyDocument3 pagesBackground and PathophysiologyspiritNo ratings yet
- HydrocephalusDocument39 pagesHydrocephalusspiritNo ratings yet
- HYDRO 2023 International: Nit Warangal, IndiaDocument2 pagesHYDRO 2023 International: Nit Warangal, IndiaBhargava ReddyNo ratings yet
- FERC Radial Gate Inspection Report GuidanceDocument20 pagesFERC Radial Gate Inspection Report GuidanceAbhay ThakurNo ratings yet
- Stress in The WorkplaceDocument10 pagesStress in The WorkplaceWendyLu32100% (1)
- Challenges in Modern HRMDocument25 pagesChallenges in Modern HRMvineet sarawagi64% (11)
- PSP Films & ResourcesDocument24 pagesPSP Films & ResourcesThe Paradigm Shift ProjectNo ratings yet
- Mini ProjectDocument14 pagesMini ProjectEli Body ButterNo ratings yet
- HIST2601 HSienaDocument6 pagesHIST2601 HSienaQuinn HarringtonNo ratings yet
- Blood Componant Therapy (Autosaved)Document47 pagesBlood Componant Therapy (Autosaved)drkapiltNo ratings yet
- Root-Knot and Root-Lesion Nematode SuppressionDocument6 pagesRoot-Knot and Root-Lesion Nematode SuppressionRAMIRO H.S.No ratings yet
- Mole Calculation Worksheet: Practice & SolutionsDocument3 pagesMole Calculation Worksheet: Practice & SolutionsQurrat Ul AinNo ratings yet
- 16 Distillation NotesDocument6 pages16 Distillation Notesyown silvaNo ratings yet
- Preparation of nursery and seed bedsDocument7 pagesPreparation of nursery and seed bedsShree PinnintiNo ratings yet
- BCM Action PlanDocument3 pagesBCM Action PlankrovvidiprasadaraoNo ratings yet
- MDocument47 pagesMKumara55No ratings yet
- Lady Wachter's Cult of Darkness InvestigationDocument11 pagesLady Wachter's Cult of Darkness InvestigationWellington Valentin100% (1)
- GOVT - Departments - Contact - Details - MF-14-06-2021 UpdatedDocument32 pagesGOVT - Departments - Contact - Details - MF-14-06-2021 Updatedadf_raghuNo ratings yet
- 15419Document29 pages15419Sadashiva SahooNo ratings yet
- Grand Rounds 183068 7Document46 pagesGrand Rounds 183068 7Nada PetrovićNo ratings yet
- Dr. P S Adhya 7186Document1 pageDr. P S Adhya 7186Partha AdhyaNo ratings yet
- Instruction: 217 - C Fiber Optic Splice CaseDocument9 pagesInstruction: 217 - C Fiber Optic Splice CaseHữu Khánh NguyễnNo ratings yet
- Uwezo-SAT-W-L-In Class-SET 1 - WMDocument15 pagesUwezo-SAT-W-L-In Class-SET 1 - WMAditya KantipudiNo ratings yet
- Clay Types PDFDocument40 pagesClay Types PDFHafiz Mudaser AhmadNo ratings yet
- Long-Term Memory - ProcessDocument30 pagesLong-Term Memory - ProcessALEXANDRA SAN PEDRONo ratings yet
- Bukidnon's Top Food, Nature SitesDocument3 pagesBukidnon's Top Food, Nature SitesslumbaNo ratings yet
- Trix Price List OCT 2018 PDFDocument2 pagesTrix Price List OCT 2018 PDFApNo ratings yet
- SS - 578 - 2012 - Use and Maintenance of Fire ExtinguishersDocument24 pagesSS - 578 - 2012 - Use and Maintenance of Fire Extinguishersrasanavaneethan100% (4)
- Astm E1973 - 1 (En)Document4 pagesAstm E1973 - 1 (En)Dinesh SaiNo ratings yet
- Strack 1976 A Single-Potential Solution For Regional Interface Problems in Coastal AquifersDocument10 pagesStrack 1976 A Single-Potential Solution For Regional Interface Problems in Coastal AquifersMarie.NeigeNo ratings yet
- Pharma AssignDocument8 pagesPharma AssignTHIS PAHADINo ratings yet
- The Abreviated Ajahn Brahm - Concise Instructions For Skillful Meditation PDFDocument8 pagesThe Abreviated Ajahn Brahm - Concise Instructions For Skillful Meditation PDFJean Bessaudou Jan BessNo ratings yet