You might also like
- Ab IdentificationDocument74 pagesAb IdentificationMai HanyNo ratings yet
- Ab Screening PDFDocument67 pagesAb Screening PDFJerome ValerianoNo ratings yet
- DR - Usi-Screening & Identification AntibodyDocument44 pagesDR - Usi-Screening & Identification AntibodySukma EffendyNo ratings yet
- Pre Transfusion TestingDocument67 pagesPre Transfusion TestingPaulino GarciaNo ratings yet
- Detection and Identification of Antibodies - SCDocument67 pagesDetection and Identification of Antibodies - SCLyra Dennise LlidoNo ratings yet
- Antibody Screening and IDDocument60 pagesAntibody Screening and IDPamela MendozaNo ratings yet
- Walmart Global Sourcing - Improve - & - ControlDocument27 pagesWalmart Global Sourcing - Improve - & - Controlmagudeesh100% (1)
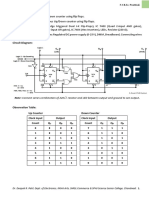
- SY - Synchronous Counter Using Flip FlopsDocument2 pagesSY - Synchronous Counter Using Flip FlopsAbhishek ParmarNo ratings yet
- Chapter #5: Programmable Logic ControllerDocument30 pagesChapter #5: Programmable Logic ControllerPavi TranNo ratings yet
- 2 Raos ISBT Immunohematology WP Case Study 1 FINAL PDFDocument31 pages2 Raos ISBT Immunohematology WP Case Study 1 FINAL PDFdrtsotlhe mogolegwaNo ratings yet
- Computer Servicing 4: Introduction To Logic Gates Boolean AlgebraDocument13 pagesComputer Servicing 4: Introduction To Logic Gates Boolean AlgebraJhon Keneth NamiasNo ratings yet
- Advanced Immunohematology TechniquesDocument47 pagesAdvanced Immunohematology TechniquesPamela MendozaNo ratings yet
- How Many Absences in School Do You Commit in A WeekDocument3 pagesHow Many Absences in School Do You Commit in A WeekRoselle BarcelonNo ratings yet
- 2019-01-23 - HiPEAC Tutorial - AritraDocument30 pages2019-01-23 - HiPEAC Tutorial - AritraAritra SarkarNo ratings yet
- PCB Reprt (1) FinalDocument8 pagesPCB Reprt (1) FinalShamma SNo ratings yet
- CELEBROWDocument16 pagesCELEBROWEpaja Jeremiah JesseNo ratings yet
- Biodiversity Questions Vs Schemes (Totals (Others Hidden) )Document5 pagesBiodiversity Questions Vs Schemes (Totals (Others Hidden) )Matias JaraNo ratings yet
- Problem Table Algorithm: Company NameDocument1 pageProblem Table Algorithm: Company NameGiussepi Ali Jhonatan Mamani PacoNo ratings yet
- Problem Table Algorithm: Company NameDocument1 pageProblem Table Algorithm: Company NameGloria Elena PerezNo ratings yet
- BMA Lab Report Digital IIDocument7 pagesBMA Lab Report Digital IIAmine usmaNo ratings yet
- Grade83rdQuarterSummativeTest-2024-03-24T13_14_57_462041-46399cDocument12 pagesGrade83rdQuarterSummativeTest-2024-03-24T13_14_57_462041-46399clabiosjasminNo ratings yet
- Malaria 19 NewDocument106 pagesMalaria 19 NewmeckhyseranNo ratings yet
- Solución de problemas de estructuras 1Document12 pagesSolución de problemas de estructuras 1Jose Jean Ramos SerranoNo ratings yet
- Indra Bulan JuniDocument4 pagesIndra Bulan JuniLaeli NurmaeniNo ratings yet
- 3-bit asynchronous Up/Down counter flip-flopsDocument2 pages3-bit asynchronous Up/Down counter flip-flopsIshtiaque Ahmed TanimNo ratings yet
- Demp Session - 2 VPDocument65 pagesDemp Session - 2 VPRAHUL KUMAR RNo ratings yet
- SR .No. Name of Sheet StatusDocument6 pagesSR .No. Name of Sheet StatusMaheswaraRaoNo ratings yet
- Assignment 1 DSE 163Document4 pagesAssignment 1 DSE 163sandunmaheesha01No ratings yet
- TallerDocument2 pagesTallerEmily Belén Aguilar VeraNo ratings yet
- 320 Into Binary:: Introduction To Computing (CS101)Document3 pages320 Into Binary:: Introduction To Computing (CS101)Hohaho YohahaNo ratings yet
- Ex No:4 Code Convertors: CS2207-Digital LabDocument7 pagesEx No:4 Code Convertors: CS2207-Digital LabSuresh Babu PalpandiNo ratings yet
- Activity 1 - Logicgates WorksheetDocument5 pagesActivity 1 - Logicgates Worksheetmirror100% (1)
- Experiment No 18Document4 pagesExperiment No 18NEAYZ AHMADNo ratings yet
- Ms Data 2004-2Document47 pagesMs Data 2004-2seenuNo ratings yet
- E91 IntroDocument25 pagesE91 IntroAlekso GjakovskiNo ratings yet
- Assement 04Document5 pagesAssement 04Naina PrasharNo ratings yet
- 0008-BSCS-19 MUHAMMAD JUNAID TARIQ (DLD Lab) Word FileDocument6 pages0008-BSCS-19 MUHAMMAD JUNAID TARIQ (DLD Lab) Word FileKashif KashifNo ratings yet
- Cse 206 - Lab 05Document4 pagesCse 206 - Lab 05Syed IrfanNo ratings yet
- MP TB ListDocument7 pagesMP TB ListNakka Srikanth RajNo ratings yet
- Format Pelaporan Logistik NonARV 2022 - Rev LAYANAN MEDANDocument6 pagesFormat Pelaporan Logistik NonARV 2022 - Rev LAYANAN MEDANJava GreenNo ratings yet
- MalariaDocument130 pagesMalariainamulyatiumbunayNo ratings yet
- Laporan Diagnosis February 2024Document3 pagesLaporan Diagnosis February 2024muhammad sudrajatNo ratings yet
- Indera Bulan MeiDocument4 pagesIndera Bulan MeiLaeli NurmaeniNo ratings yet
- 0001 Introduction SpiceDocument9 pages0001 Introduction SpiceRimsha pervaizNo ratings yet
- LepraDocument164 pagesLepraEng AtawoloNo ratings yet
- Daily HW Log ErpDocument9 pagesDaily HW Log Erpm.boswellNo ratings yet
- Laporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuDocument37 pagesLaporan Bulanan Rekapitulasi Surveilans Terpadu Penyakit (STP) Baru Di Puskesmas Dan Jejaringnya Puskesmas SoliuVictoria YanersNo ratings yet
- Binary Numbers and Conversions ChartDocument5 pagesBinary Numbers and Conversions ChartShubh MerjaNo ratings yet
- Sensus Imn 2021Document48 pagesSensus Imn 2021elga lesmanaNo ratings yet
- Capter 5Document53 pagesCapter 5surafel5248No ratings yet
- Laporan Pws Penyakit 16032022surveilancefeb22Document4 pagesLaporan Pws Penyakit 16032022surveilancefeb22Covid petamburanNo ratings yet
- Ketogenic Diet Meal Planner: Enter FoodDocument3 pagesKetogenic Diet Meal Planner: Enter FoodsimasNo ratings yet
- Binary Addition and SubtractionDocument3 pagesBinary Addition and SubtractionRiaz KhanNo ratings yet
- VERIFICATIONDocument7 pagesVERIFICATIONNOV DAVANNNo ratings yet
- Sensus Juli 2021Document52 pagesSensus Juli 2021Bonita PrimaNo ratings yet
- Multi-body dynamics modelDocument1 pageMulti-body dynamics modelLina Stella Forigua AndradeNo ratings yet
- Autoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Document5 pagesAutoimmune - Hemolytic - Anemia - Mixed - Type-A - Case - Repo 2Afsha AnishNo ratings yet
- Congenital and Aquired Hemolytic Anemias QuestionsDocument36 pagesCongenital and Aquired Hemolytic Anemias QuestionstoniassafNo ratings yet
- Autoimmune Hemolytic Anemia in Adults 2019 PDFDocument22 pagesAutoimmune Hemolytic Anemia in Adults 2019 PDFKevin Mora BañosNo ratings yet
- 4 5913696519462061514 PDFDocument248 pages4 5913696519462061514 PDFcristhian urquizoNo ratings yet
- HypersensitivityDocument20 pagesHypersensitivityJAIRA RIEYELLE LIPANANo ratings yet
- Emergency transfusion guidelines for AIHA patientsDocument5 pagesEmergency transfusion guidelines for AIHA patientspriscilla harmanyNo ratings yet
- Red blood cell abnormalities revealedDocument39 pagesRed blood cell abnormalities revealedShishir AhmedNo ratings yet
- Experiment #10: Direct Antihuman Globulin Test: ReferenceDocument8 pagesExperiment #10: Direct Antihuman Globulin Test: ReferenceKriziaNo ratings yet
- Normocytic Normochromic AnemiaDocument18 pagesNormocytic Normochromic AnemiaElaizha PagulayanNo ratings yet
- CC2H G Raines - What Are Cryo-Proteins and How Do You Test For ThemDocument31 pagesCC2H G Raines - What Are Cryo-Proteins and How Do You Test For ThemSaad KhanNo ratings yet
- 2.13.08 Cold Agglutinin RogersDocument27 pages2.13.08 Cold Agglutinin RogersJessica StewartNo ratings yet
- BB Lec13 AihaDocument11 pagesBB Lec13 AihaLem obadNo ratings yet
- Autoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisDocument10 pagesAutoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisMARCO MONTES REYESNo ratings yet
- Boc Immunology PDFDocument53 pagesBoc Immunology PDFLIANNE RAMIREZNo ratings yet
- Mindray Enhanced Training For Applications Cme-MetaDocument20 pagesMindray Enhanced Training For Applications Cme-MetaSkylake CoffeelakeNo ratings yet
- Blood Reviews: ReviewDocument22 pagesBlood Reviews: ReviewJair Alexander Quintero PanucoNo ratings yet
- Autoimmune Hemolytic Anemia: Anita Hill and Quentin A. HillDocument8 pagesAutoimmune Hemolytic Anemia: Anita Hill and Quentin A. HillRahmawati HamudiNo ratings yet
- Pediatrics CLINICAL QUESTIONDocument14 pagesPediatrics CLINICAL QUESTIONAyesha KhatunNo ratings yet
- Bloodbld 2019003808 CDocument12 pagesBloodbld 2019003808 CBillal BenhaddadNo ratings yet
- Antibody PanelDocument81 pagesAntibody PanelMa. Pe Delaine MendrosNo ratings yet
- GLOSSARY MEDICAL TERMSDocument83 pagesGLOSSARY MEDICAL TERMSLim Hui ZhuanNo ratings yet
- Utoimmune Hemolytic Anemia: Reported By: Kathleen Chris G. Lapac MLS 3-ADocument11 pagesUtoimmune Hemolytic Anemia: Reported By: Kathleen Chris G. Lapac MLS 3-AABHINABA GUPTANo ratings yet
- IMXv6!1!07B Hematology II Anemia Disorders of Red Blood Cells PartDocument12 pagesIMXv6!1!07B Hematology II Anemia Disorders of Red Blood Cells PartChurschmann SpiralNo ratings yet
- SMLLDocument8 pagesSMLLArifa Al HusnahNo ratings yet
- Immunohematology MCQsDocument21 pagesImmunohematology MCQsMeerva El-zein86% (21)
- RBC Disorder BcqsDocument68 pagesRBC Disorder BcqsMukhtiar AhmedNo ratings yet
- New Insights in The Pathogenesis and Therapy of Cold Agglutinin-Mediated Autoimmune Hemolytic AnemiaDocument13 pagesNew Insights in The Pathogenesis and Therapy of Cold Agglutinin-Mediated Autoimmune Hemolytic AnemiaKadek AyuNo ratings yet
- Is FinalsDocument78 pagesIs FinalsMarissa CordovaNo ratings yet
- Hematology and Clinical Microscopy Glossary GuideDocument104 pagesHematology and Clinical Microscopy Glossary GuideJancarlos Cesar CondorNo ratings yet
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocument500 pagesSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNo ratings yet