You might also like
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 pagesObstetric Anal Sphincter Injury (OASIS) - UpToDateErickNo ratings yet
- Handbook of Current and Novel Protocols for the Treatment of InfertilityFrom EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNo ratings yet
- Cardiac Disease in PregnancyDocument28 pagesCardiac Disease in PregnancyviharadewiNo ratings yet
- Dystocia and Augmentation of LAbor PDFDocument10 pagesDystocia and Augmentation of LAbor PDFKathleenNo ratings yet
- Mal Positions / Mal PresentationsDocument21 pagesMal Positions / Mal PresentationsSatyendra Batra100% (2)
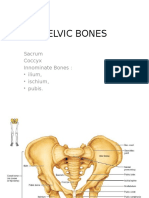
- Pelvic BoneDocument15 pagesPelvic BoneYoanneveline TanakNo ratings yet
- Cervical CancerDocument30 pagesCervical Cancerhuhknee100% (1)
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocument10 pages(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Spontaneous Delivery in Post-Term PregnancyDocument55 pagesSpontaneous Delivery in Post-Term Pregnancyr.pavinvikneshNo ratings yet
- VTE in Pregnancy 2021 by DR AmanuelDocument43 pagesVTE in Pregnancy 2021 by DR AmanuelAmanuel We/gebriel100% (1)
- National Rural Health MissionDocument418 pagesNational Rural Health MissionRoy GoldenNo ratings yet
- Claire Maevelle A. Laxamana BSP - 3ADocument10 pagesClaire Maevelle A. Laxamana BSP - 3ACLaire Maevelle Angeles LaxamanaNo ratings yet
- Abnormalities of Amniotic FluidDocument32 pagesAbnormalities of Amniotic FluidMuhammad Abdillah100% (1)
- Exclusive BreastfeedingDocument1 pageExclusive BreastfeedingLeah BancaleNo ratings yet
- Complicated Labor and DeliveryDocument226 pagesComplicated Labor and Deliveryrhimineecat71100% (1)
- Cardiac Disease in PregnancyDocument21 pagesCardiac Disease in PregnancyRenata CilestrinaNo ratings yet
- Obstetric EmergenciesDocument28 pagesObstetric EmergenciesRina Fatimah NurillahNo ratings yet
- Update Iugr Classification 2014Document13 pagesUpdate Iugr Classification 2014NidhaSavitriNo ratings yet
- Gestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Document13 pagesGestational Trophoblastic Disease (Neha Martin Msc. NSG 2nd Year)Gunu SinghNo ratings yet
- PDFDocument8 pagesPDFSaumya SharmaNo ratings yet
- Miscarriage Early Pregnancy LossDocument10 pagesMiscarriage Early Pregnancy LossiwennieNo ratings yet
- Question Bank: Paper 3 - Organisation of Hospital ServicesDocument5 pagesQuestion Bank: Paper 3 - Organisation of Hospital ServicesDr. Rakshit SolankiNo ratings yet
- Cryo SurgeryDocument8 pagesCryo SurgeryninroseNo ratings yet
- Obstetrical Hemorrhage: Reynold John D. ValenciaDocument82 pagesObstetrical Hemorrhage: Reynold John D. ValenciaReynold John ValenciaNo ratings yet
- Classification of Obstetric Shock Diagnosis and MonitoringDocument3 pagesClassification of Obstetric Shock Diagnosis and MonitoringAryo PraditoNo ratings yet
- Disorders During PregnancyDocument12 pagesDisorders During PregnancyazlanNo ratings yet
- Ambulatory HysterosDocument8 pagesAmbulatory Hysteroskomlanihou_890233161100% (1)
- The Nurses and Midwives Act No. 10 of 2019. PMDDocument43 pagesThe Nurses and Midwives Act No. 10 of 2019. PMDhfcvbNo ratings yet
- Anatomy of Female Genital Tract by Sidra IftikharDocument33 pagesAnatomy of Female Genital Tract by Sidra IftikharWaqas Tahir100% (1)
- RCOG Cardiac Disease and Pregnancy PDFDocument18 pagesRCOG Cardiac Disease and Pregnancy PDFSteven SetioNo ratings yet
- The Nigeria Police Force Schedule of Duty-1Document69 pagesThe Nigeria Police Force Schedule of Duty-1ABDULSALAM SADIQ AMINUNo ratings yet
- GEN GallBladderInstrumentsADocument10 pagesGEN GallBladderInstrumentsANeo Rodriguez AlvaradoNo ratings yet
- 1-Cardiac Disease With PregnancyDocument46 pages1-Cardiac Disease With PregnancyDrMohammad KhadrawyNo ratings yet
- Gestational Trophoblastic DiseaseDocument6 pagesGestational Trophoblastic DiseaseSJ IraaNo ratings yet
- Investigation InfertilityDocument44 pagesInvestigation InfertilityDenisNo ratings yet
- Bench MarkingDocument16 pagesBench MarkingNorj BaraniNo ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- Fetal Growth Restriction - ACOG 2019Document23 pagesFetal Growth Restriction - ACOG 2019Adhitya Yudha MaulanaNo ratings yet
- Anatomy Physiology PregnancyDocument45 pagesAnatomy Physiology PregnancyFilbertaNo ratings yet
- Sepsis Management PDFDocument118 pagesSepsis Management PDFsarita julia putriNo ratings yet
- Vesicular MoleDocument46 pagesVesicular Molekhadzx100% (2)
- GTG 37bDocument32 pagesGTG 37bKadelsy BristolNo ratings yet
- Sepsis in Peg Rcog PDFDocument14 pagesSepsis in Peg Rcog PDFSapna SNo ratings yet
- Postnatal Care PDFDocument9 pagesPostnatal Care PDFYanti PoltekkesNo ratings yet
- FGM Awareness PowerpointDocument10 pagesFGM Awareness Powerpointapi-403276113No ratings yet
- Renal Disease in PregnancyDocument28 pagesRenal Disease in PregnancysuperjaxxxonNo ratings yet
- Ovarian Cancer SGTDocument25 pagesOvarian Cancer SGTAndre PutraNo ratings yet
- Ectopic Pregnancy PDFDocument38 pagesEctopic Pregnancy PDFByron Ruiz Lapuerta100% (1)
- Open Disclosure Principles Elements and ProcessDocument11 pagesOpen Disclosure Principles Elements and ProcessRedroses flowersNo ratings yet
- AnestesiDocument15 pagesAnestesiayang rasheldaNo ratings yet
- Kehamilan MolaDocument88 pagesKehamilan MolaYhanna UlfianiNo ratings yet
- The Chinese University of Hong Kong Obstetrics and Gynaecology Module Student Handbook 2016-2017Document37 pagesThe Chinese University of Hong Kong Obstetrics and Gynaecology Module Student Handbook 2016-2017Ken100% (1)
- DysmenorrheaDocument8 pagesDysmenorrheasalamredNo ratings yet
- Post Partum Haem.Document90 pagesPost Partum Haem.rachael annor100% (1)
- MSI Guidelines For Obstetric Care v2.0Document295 pagesMSI Guidelines For Obstetric Care v2.0Daniel AbomaNo ratings yet
- Pregnancy Kidney DiseaseDocument18 pagesPregnancy Kidney DiseaseMihai PavaleanNo ratings yet
- CENTER'S IMPLANT COURSEDocument4 pagesCENTER'S IMPLANT COURSEadel abdelmageedNo ratings yet
- BMG UrethroplastyDocument47 pagesBMG UrethroplastyMekbeb ChereNo ratings yet
- Rare Case of Spontaneous Renal Pelvis Rupture from Ureteral StoneDocument6 pagesRare Case of Spontaneous Renal Pelvis Rupture from Ureteral StoneMekbeb ChereNo ratings yet
- Metabolic Abnormalities in Urinary Diversion Using IntestineDocument16 pagesMetabolic Abnormalities in Urinary Diversion Using IntestineMekbeb ChereNo ratings yet
- Assesing Renal Function Using Contrast CTDocument22 pagesAssesing Renal Function Using Contrast CTMekbeb ChereNo ratings yet
- Continious Saline Irrigation After TURBT For NMIBCDocument10 pagesContinious Saline Irrigation After TURBT For NMIBCMekbeb ChereNo ratings yet
- List of Super Specialty Treatment (SST) Tie Up Hospitals in West Bengal For The Year 2016-20181Document6 pagesList of Super Specialty Treatment (SST) Tie Up Hospitals in West Bengal For The Year 2016-20181Arijit MondalNo ratings yet
- Plastic Surgery Vs Natural BeautyDocument15 pagesPlastic Surgery Vs Natural Beautymoneeka lodhaNo ratings yet
- Acuan Tarif Jasa Medik Dokter (IDI)Document214 pagesAcuan Tarif Jasa Medik Dokter (IDI)kiyoeugraNo ratings yet
- Case Log Coding Guidelines: Review Committee For Otolaryngology AcgmeDocument21 pagesCase Log Coding Guidelines: Review Committee For Otolaryngology AcgmeJonathan C. SimmondsNo ratings yet
- About Noble - 11Document3 pagesAbout Noble - 11Anonymous AnmGhjCNo ratings yet
- DR Afwan Fajri - Trauma - Juli 2023Document82 pagesDR Afwan Fajri - Trauma - Juli 2023afwan fajriNo ratings yet
- Nrutik Paper 22Document6 pagesNrutik Paper 22Nrutik PatelNo ratings yet
- Ortho FractureDocument2 pagesOrtho FractureFritzTarronasNo ratings yet
- Surgical Treatment of Talus Fractures PDFDocument9 pagesSurgical Treatment of Talus Fractures PDFumesh sarojNo ratings yet
- NephroptosisDocument10 pagesNephroptosisaabbccss1.z71No ratings yet
- Aetna Clinics - SingaporeDocument51 pagesAetna Clinics - Singaporergopalan0% (1)
- Jurnal Tentang Intervensi Keperawatan: Pedoman Penyusunan Laporan Presentasi JurnalDocument2 pagesJurnal Tentang Intervensi Keperawatan: Pedoman Penyusunan Laporan Presentasi JurnalDesilvaNo ratings yet
- Penetrating Abdominal Trauma ManagementDocument27 pagesPenetrating Abdominal Trauma ManagementhoangducnamNo ratings yet
- Urogynecology Case SummariesDocument4 pagesUrogynecology Case SummariesDwickyNo ratings yet
- Clinical Assessment of Abdominal TraumaDocument77 pagesClinical Assessment of Abdominal Traumaummu husnaNo ratings yet
- Meuthia Describing WoundsDocument3 pagesMeuthia Describing WoundsMuthia MauliddaNo ratings yet
- Case2CaseMedicalDoctorsDocument2 pagesCase2CaseMedicalDoctorsedkattaNo ratings yet
- ATLS Course Schedule for Doctors in Palembang, IndonesiaDocument3 pagesATLS Course Schedule for Doctors in Palembang, IndonesiaNamira Firdha KesumaNo ratings yet
- Disease) and Serious Kidney Infections. ItDocument3 pagesDisease) and Serious Kidney Infections. ItKarlo DifuntorumNo ratings yet
- Plastic Surgery and Physiotherapy GuideDocument3 pagesPlastic Surgery and Physiotherapy GuideGanga S GovindNo ratings yet
- CGHS RATE List PDFDocument42 pagesCGHS RATE List PDFNarain Kumar LangehNo ratings yet
- Blefaroplastia Superior Associada A Remoção de Pele Abaixo Do Supercílio em Pacientes de Origem AsiaticaDocument4 pagesBlefaroplastia Superior Associada A Remoção de Pele Abaixo Do Supercílio em Pacientes de Origem AsiaticaIvoNo ratings yet
- Status Pasien Ruang ICU dan Ruang Perawatan BTKV Kamis, 14 Juli 2022Document9 pagesStatus Pasien Ruang ICU dan Ruang Perawatan BTKV Kamis, 14 Juli 2022Arif KurniawanNo ratings yet
- Regional Traumatology of the AnkleDocument18 pagesRegional Traumatology of the AnkleNiroshni SusanNo ratings yet
- Ocular TraumaDocument19 pagesOcular TraumaUmar AzlanNo ratings yet
- FracturesDocument20 pagesFracturesSanam MalikNo ratings yet
- Jarvis 2012 Practical UroflowmetryDocument2 pagesJarvis 2012 Practical UroflowmetryFoxglove83No ratings yet
- Grs 2021 00059Document8 pagesGrs 2021 00059jonj72351No ratings yet
- NCP Urinary RetentionDocument3 pagesNCP Urinary RetentionKingJayson Pacman06No ratings yet
- Januari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFDocument2 pagesJanuari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFVirly EffendiNo ratings yet