You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MDS Oral Medicine Question Papers 2002Document5 pagesMDS Oral Medicine Question Papers 2002Niyas UmmerNo ratings yet
- Upstream CAE Test 7Document3 pagesUpstream CAE Test 7adevoicuNo ratings yet
- ABNORMAL Drill Week2Document8 pagesABNORMAL Drill Week2MS Zhou Si ViolonNo ratings yet
- Sample - Drug Index DatabaseDocument12 pagesSample - Drug Index DatabaseEubert John VenturinaNo ratings yet
- Pediatric Board Review Multiple Choice Questions - 2012 - 09!20!23!25!29 - 296Document51 pagesPediatric Board Review Multiple Choice Questions - 2012 - 09!20!23!25!29 - 296Ayman Kafosid90% (51)
- Orthodontic Management in Children With Special NeedsDocument5 pagesOrthodontic Management in Children With Special NeedsAnonymous LnWIBo1GNo ratings yet
- Basic Surgical Techniques For Endosseous Implant PlacementDocument101 pagesBasic Surgical Techniques For Endosseous Implant PlacementAnshuman Dwivedi100% (2)
- Vertigo For GP - How To Approach It - Dr. Ni Nengah Rida AriariniDocument21 pagesVertigo For GP - How To Approach It - Dr. Ni Nengah Rida AriariniAsiatiNo ratings yet
- Dr. Waluyo Rudiyanto, M.KesDocument50 pagesDr. Waluyo Rudiyanto, M.KesAsiatiNo ratings yet
- Furo Menu A4 Compressed 2 1Document17 pagesFuro Menu A4 Compressed 2 1AsiatiNo ratings yet
- Update On Systemic Glucocorticosteroids in Dermatology: C. MD, T. MDDocument15 pagesUpdate On Systemic Glucocorticosteroids in Dermatology: C. MD, T. MDAsiatiNo ratings yet
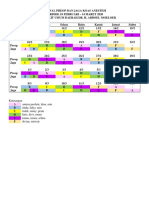
- JADWAL KOAS ANESTESI 10 Feb - 14 MarDocument2 pagesJADWAL KOAS ANESTESI 10 Feb - 14 MarAsiatiNo ratings yet
- Alamanda'S 2 Floor: Rifqi Fadhil M Helen Kusuma WDocument4 pagesAlamanda'S 2 Floor: Rifqi Fadhil M Helen Kusuma WAsiatiNo ratings yet
- Skin To SkinDocument9 pagesSkin To SkinAsiatiNo ratings yet
- DO - Public Speaking (Dr. Dwita Oktaria, M.PD - Ked.)Document42 pagesDO - Public Speaking (Dr. Dwita Oktaria, M.PD - Ked.)AsiatiNo ratings yet
- 23 Agt InggrisDocument17 pages23 Agt InggrisAsiatiNo ratings yet
- 1 PB PDFDocument10 pages1 PB PDFAsiatiNo ratings yet
- CV MR Dec19Document6 pagesCV MR Dec19AsiatiNo ratings yet
- The Relationship Between The Big Five Personality Factors With Blood Types inDocument8 pagesThe Relationship Between The Big Five Personality Factors With Blood Types inAsiatiNo ratings yet
- Drug Use in Nigeria: ResearchDocument61 pagesDrug Use in Nigeria: ResearchalexNo ratings yet
- TEACHER-Made-Learners-Home-Task Nailcare 3Document4 pagesTEACHER-Made-Learners-Home-Task Nailcare 3Marjune RedondoNo ratings yet
- Nephro Gudie For HODocument22 pagesNephro Gudie For HOSarmad AsifNo ratings yet
- What Is CardiomyopathyDocument8 pagesWhat Is CardiomyopathysakuraleeshaoranNo ratings yet
- Birth Asphycia and Cerebral Palsy Clinics Perinatology 2005Document16 pagesBirth Asphycia and Cerebral Palsy Clinics Perinatology 2005Sebastián Silva SotoNo ratings yet
- Get The Facts About COVID-19 Vaccines - Mayo ClinicDocument10 pagesGet The Facts About COVID-19 Vaccines - Mayo ClinicLuna BellatrixNo ratings yet
- Seminar Kasus RDSDocument16 pagesSeminar Kasus RDSIntan agustinNo ratings yet
- C. HPCT File Week 1 Introduction To General Pathology and HistoTechniquesDocument32 pagesC. HPCT File Week 1 Introduction To General Pathology and HistoTechniquesAliah Anne MagnoNo ratings yet
- Mottling Score - ICM 2011Document7 pagesMottling Score - ICM 2011cyelzNo ratings yet
- K - 2 Secondary Survey Assessment (Anestesi)Document39 pagesK - 2 Secondary Survey Assessment (Anestesi)AndreAHutasoitNo ratings yet
- Phlebotomy and Specimen ConsiderationsDocument21 pagesPhlebotomy and Specimen ConsiderationsLesly Marie LaxamanaNo ratings yet
- Antimicrobial Sensitivity of Most Commonly Isolated Bacteria From Feline Upper Respiratory Infection (URI)Document3 pagesAntimicrobial Sensitivity of Most Commonly Isolated Bacteria From Feline Upper Respiratory Infection (URI)KAREN LEE MEI FONGNo ratings yet
- Phenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsDocument2 pagesPhenylephrine: 1568 Cough Suppressants Expectorants Mucolytics and Nasal DecongestantsRanny LaidasuriNo ratings yet
- Assessing Blood PressureDocument4 pagesAssessing Blood PressureCraigyyNo ratings yet
- International HIV & AIDS Charity Donate Fundraising About AVERT AIDS Projects Help & Advice Contact Us Facebook NewsletterDocument22 pagesInternational HIV & AIDS Charity Donate Fundraising About AVERT AIDS Projects Help & Advice Contact Us Facebook NewsletterbasmashaddadNo ratings yet
- Concept MapDocument9 pagesConcept Mapsinai1012No ratings yet
- Nursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleDocument6 pagesNursing Test Bank Introductory Mental Health Nursing 2nd Edition by Donna M WombleHarry Coston100% (35)
- Adrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianDocument13 pagesAdrenal Gland Disease in Ferrets: Elisabeth Simone-Freilicher, DVM, DABVP-AvianGabriel MendesNo ratings yet
- Do Vaccinations Cause Autism?Document3 pagesDo Vaccinations Cause Autism?Josh BarberaNo ratings yet
- Mood Disorder and SuicideDocument58 pagesMood Disorder and SuicideMichael AsetreNo ratings yet
- Clinical Handbook of Infectious Diseases in Farm AnimalsDocument146 pagesClinical Handbook of Infectious Diseases in Farm Animalsigorgalopp100% (1)
- ExamDocument50 pagesExamSyeda Eshaal JavaidNo ratings yet
- Holid Fauzi, Suningsih, Setyo Adi NugrohoDocument6 pagesHolid Fauzi, Suningsih, Setyo Adi NugrohoKholifatun NaziroNo ratings yet