You might also like
- Books For ZNO Your Personality and You Workbook Yael H Dubin MD PDFDocument167 pagesBooks For ZNO Your Personality and You Workbook Yael H Dubin MD PDFДанілова Тетяна100% (1)
- A Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Skin Fungal Infections, (Updated 2023) Diagnosis, Treatment and Related ConditionsRating: 5 out of 5 stars5/5 (2)
- Promoting Student HappinessDocument289 pagesPromoting Student HappinessMarie MalcampoNo ratings yet
- Arnold Jacobs On BreathingDocument5 pagesArnold Jacobs On Breathingscriberone100% (1)
- Draft ISO 45001 GuideDocument15 pagesDraft ISO 45001 GuideCristian Camilo Rodriguez93% (15)
- Positive Psychology PDFDocument4 pagesPositive Psychology PDFoooocanada100% (1)
- General Considerations For Topical PreparationsDocument6 pagesGeneral Considerations For Topical PreparationsOccamsRazorNo ratings yet
- Harness Performance With Assays Designed For Your LaboratoryDocument4 pagesHarness Performance With Assays Designed For Your LaboratoryDjajanan KoreaNo ratings yet
- Athlete's Foot (Tinea Pedis)Document21 pagesAthlete's Foot (Tinea Pedis)farmasi_hm100% (1)
- Personal Notes On TineaDocument35 pagesPersonal Notes On TineaSaleh Mohammad ShoaibNo ratings yet
- Fungal Skin InfectionsDocument30 pagesFungal Skin InfectionsfaizNo ratings yet
- Fungal Skin InfectionsDocument31 pagesFungal Skin InfectionsCareyTranNo ratings yet
- MICRODocument6 pagesMICROShaye Toliao GeligNo ratings yet
- Biofar TransdermalDocument33 pagesBiofar Transdermaledwin aldrinNo ratings yet
- Pharmacology REPORTDocument23 pagesPharmacology REPORTMaria RosaNo ratings yet
- 3) Bacterial Skin Infections Semi NotesDocument2 pages3) Bacterial Skin Infections Semi NotesIssa MoodNo ratings yet
- Study Guide Ch.11Document7 pagesStudy Guide Ch.11Draquillany ShieldsNo ratings yet
- Management of Adult PsoriasisDocument1 pageManagement of Adult PsoriasisCollective123No ratings yet
- Fungal Infections & Lulyeva Itra EvaDocument9 pagesFungal Infections & Lulyeva Itra EvaMonod TNo ratings yet
- Australian Doctor - 025 - 032 - MAR19 - 10Document6 pagesAustralian Doctor - 025 - 032 - MAR19 - 10leh.mo9315No ratings yet
- Tinea PedisDocument15 pagesTinea PedisKasujja AhmedNo ratings yet
- Poonam PPT FinalDocument15 pagesPoonam PPT Finalpooam_rktNo ratings yet
- 56-Topical Drugs Used in The Treatment of Skin DisordersDocument13 pages56-Topical Drugs Used in The Treatment of Skin DisordersMujeebNo ratings yet
- Piedraia Hortae Which Is Manifested by A Small FirmDocument5 pagesPiedraia Hortae Which Is Manifested by A Small FirmMnemo SyneNo ratings yet
- FungiDocument3 pagesFungikrystal TortolaNo ratings yet
- Anthelmintic DrugsDocument1 pageAnthelmintic DrugsShrenil LagadNo ratings yet
- L-1 Anti FungalsDocument10 pagesL-1 Anti Fungalsigrg382No ratings yet
- About The Diseases: Foot RotDocument2 pagesAbout The Diseases: Foot RotsasmitaNo ratings yet
- Topical CorticosteroidsDocument1 pageTopical CorticosteroidsDavid HosamNo ratings yet
- Pengendalian Hama GudangDocument24 pagesPengendalian Hama GudangYudha Pradhana PNo ratings yet
- Topical Protectives: Group 5 Haboc, Bea Armaine Herrella, Hannah Marie Inumerable, Myzhel Jain, Natasha Kobayashi, TacttoDocument8 pagesTopical Protectives: Group 5 Haboc, Bea Armaine Herrella, Hannah Marie Inumerable, Myzhel Jain, Natasha Kobayashi, TacttoMyzhel InumerableNo ratings yet
- Homoeopathy An Alternative Therapy For Dermatophyte InfectionsDocument5 pagesHomoeopathy An Alternative Therapy For Dermatophyte InfectionsAman QureshiNo ratings yet
- Wound Dressings NotesDocument3 pagesWound Dressings Noteskklpuchong1717No ratings yet
- Anti-Fungl Lecture Notes As A SummaryDocument10 pagesAnti-Fungl Lecture Notes As A Summaryخالد الشرعبيNo ratings yet
- Dermasim PDFDocument3 pagesDermasim PDFSilent ScreamNo ratings yet
- Pace Partnership Wound Care ProtocolDocument5 pagesPace Partnership Wound Care ProtocolAmmar AlnajjarNo ratings yet
- Dermatofitosis PPT (Usbah, Clau, Opi)Document29 pagesDermatofitosis PPT (Usbah, Clau, Opi)NoviaPutriRahmanNo ratings yet
- Aseptic Technique: Wound Assessment On A Patient (Open or Closed)Document4 pagesAseptic Technique: Wound Assessment On A Patient (Open or Closed)AbigailNo ratings yet
- كتاب علاج الامراض الجلدية والمعدية topical preparations OTC PDF-1Document150 pagesكتاب علاج الامراض الجلدية والمعدية topical preparations OTC PDF-1ريدان عياشNo ratings yet
- Fungidal HCDocument2 pagesFungidal HCFaisal AhmedNo ratings yet
- Fungal Infection Part 2Document39 pagesFungal Infection Part 2Abaan QaisNo ratings yet
- Lecture 4Document29 pagesLecture 4ranaayy11gmailcomNo ratings yet
- Permethrin 5% Cream: Medication MOA Instruction CommentsDocument1 pagePermethrin 5% Cream: Medication MOA Instruction CommentsChron MedNo ratings yet
- Dermatophytosis ClassDocument41 pagesDermatophytosis ClassAmeena MuhammedNo ratings yet
- ANTIFUNGALSDocument11 pagesANTIFUNGALSCalvoh Asap BiketiNo ratings yet
- Managing Otitis ExternaDocument34 pagesManaging Otitis ExternaramaNo ratings yet
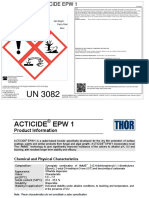
- Acticide Epw 1 2021 08 02 b02Document3 pagesActicide Epw 1 2021 08 02 b02shikaru7114No ratings yet
- Atopic Dermatitis: Aaron Justin D. TingzonDocument23 pagesAtopic Dermatitis: Aaron Justin D. TingzonChi SamaniegoNo ratings yet
- Atopic DermatitisDocument6 pagesAtopic DermatitisDr. Sarthak MishraNo ratings yet
- AdrianDocument3 pagesAdrianJohn David ZabalaNo ratings yet
- MSDS Rentokil-Klerat-EN-SDS - 01 - CHIPDocument8 pagesMSDS Rentokil-Klerat-EN-SDS - 01 - CHIPpurwadiNo ratings yet
- DermatologyDocument3 pagesDermatologyGeeta AdhikariNo ratings yet
- Plants Used To Treat Skin Diseases - ReviewDocument9 pagesPlants Used To Treat Skin Diseases - ReviewPsicólogo Clinico clinicoNo ratings yet
- Lecture-2: Pustular Diseases of The Skin and Mucous Membranes. Mycotic Skin and Mucous Membranes. Viral DermatosesDocument31 pagesLecture-2: Pustular Diseases of The Skin and Mucous Membranes. Mycotic Skin and Mucous Membranes. Viral DermatosesLatika ChoudhuryNo ratings yet
- Cypermethrin Msds 2Document5 pagesCypermethrin Msds 2FumigasiNo ratings yet
- Document 8Document2 pagesDocument 8Samantha KilaykiNo ratings yet
- Diseases Causative Agent Signs and Symptoms (3) Mode of Transmission Incubation Period Nursing Intervention With Rationale (2) Preventive MeasuresDocument5 pagesDiseases Causative Agent Signs and Symptoms (3) Mode of Transmission Incubation Period Nursing Intervention With Rationale (2) Preventive MeasuresAce FabrigasNo ratings yet
- Product and Manufacturer: Safety Data SheetDocument5 pagesProduct and Manufacturer: Safety Data SheetPurinNo ratings yet
- Nystaform OintDocument1 pageNystaform OintmahgadNo ratings yet
- 5 - Control of Microbial GrowthDocument30 pages5 - Control of Microbial GrowthAbdallah MoayadNo ratings yet
- Dermatology 2: Zienab Halem Faculty of Pharmacy SCUDocument42 pagesDermatology 2: Zienab Halem Faculty of Pharmacy SCUWijdan DaoubNo ratings yet
- Lotioncrafter: 1. Product and Company IdentificationDocument4 pagesLotioncrafter: 1. Product and Company IdentificationWangari Lothaire RachealNo ratings yet
- Methylene Chloride: Safety Data SheetDocument5 pagesMethylene Chloride: Safety Data SheetAnuj Kumar Mishra100% (1)
- Pervade 10ec SdsDocument4 pagesPervade 10ec Sdsctidalgo22No ratings yet
- MSDS GOFOS - PowderDocument8 pagesMSDS GOFOS - PowderLuan NguyenNo ratings yet
- Intertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Jury of Their Peers A Meta-Analysis of The Effects of Teen Court On Criminal RecidivismDocument16 pagesA Jury of Their Peers A Meta-Analysis of The Effects of Teen Court On Criminal RecidivismDark SiriusNo ratings yet
- Lip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndDocument20 pagesLip Posture and Its Signi Ficance Treatment Plannin G: Indiamapoli., IndYeraldin EspañaNo ratings yet
- August Month VAMDocument81 pagesAugust Month VAMBhs CherwanNo ratings yet
- History Taking Nitin SethiDocument108 pagesHistory Taking Nitin SethimaghabhothiNo ratings yet
- A Method of Analysing Interview TranscriptsDocument6 pagesA Method of Analysing Interview TranscriptsCsaba OlahNo ratings yet
- Emergency DrugsDocument19 pagesEmergency DrugsAudi Kyle SaydovenNo ratings yet
- Efficacy of Airpolishing Devices Without Removal of Implantsupported Fullarch ProsthesesDocument11 pagesEfficacy of Airpolishing Devices Without Removal of Implantsupported Fullarch ProsthesesDiego Saavedra MoralesNo ratings yet
- Emily Lane ResumeDocument3 pagesEmily Lane Resumeapi-470919717No ratings yet
- Lung Dictionary Nov18 d070819Document60 pagesLung Dictionary Nov18 d070819KEZZIA MAE ABELLANo ratings yet
- Analitika: Hubungan Antara Mindfulness Dan Kesejahteraan Subjektif Mahasiswa Selama PandemiDocument12 pagesAnalitika: Hubungan Antara Mindfulness Dan Kesejahteraan Subjektif Mahasiswa Selama PandemiMr. FernandoNo ratings yet
- PPAD Vaini IndirectDocument9 pagesPPAD Vaini IndirectJesús SCNo ratings yet
- Foreign and Local LiterarureDocument6 pagesForeign and Local Literarurepia espanilloNo ratings yet
- Hazard Report Form SampleDocument2 pagesHazard Report Form Samplewelly1980okNo ratings yet
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- The Effects of CovidDocument6 pagesThe Effects of CovidMierra PatraNo ratings yet
- Pozolotina 2017Document7 pagesPozolotina 2017Stella ÁgostonNo ratings yet
- FillersDocument25 pagesFillersAishwaryaNo ratings yet
- PROFILE OF REPUTED NGO "Deepshikha Mahila Bal Utthan Samiti"Document20 pagesPROFILE OF REPUTED NGO "Deepshikha Mahila Bal Utthan Samiti"..........Silient.............No ratings yet
- Historical Perspectives of Abnormal Psychology PaperDocument8 pagesHistorical Perspectives of Abnormal Psychology PaperSalma AhmedNo ratings yet
- Nasal Cannula Weight Guide KG Instructions Nasal Cannula Is A Single Use NasalDocument94 pagesNasal Cannula Weight Guide KG Instructions Nasal Cannula Is A Single Use NasalGuillermo MartínezNo ratings yet
- What Does The Dyslexic Person FeelDocument2 pagesWhat Does The Dyslexic Person Feelapi-650935562No ratings yet
- HemangiomaDocument15 pagesHemangiomaGrace Febryanti Toding0% (1)
- SDS Admix Gel A 50Document4 pagesSDS Admix Gel A 50adelsaqqaNo ratings yet
- DLP Health 7 CotDocument6 pagesDLP Health 7 CotRONALYNNo ratings yet