You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Plain Chest X RayDocument154 pagesPlain Chest X RaySamuel Gamadey100% (3)
- Method Statement of Pipe Painting Rev02Document44 pagesMethod Statement of Pipe Painting Rev02Abdelaziz MohamedNo ratings yet
- PASSMEDICINE MCQs-RESPIRATORY MEDICINEDocument111 pagesPASSMEDICINE MCQs-RESPIRATORY MEDICINEHashim Ahmad75% (4)
- Medical Surgical Nursing: Answer: (C) "With A Pillow, Apply Pressure Against The Incision."Document5 pagesMedical Surgical Nursing: Answer: (C) "With A Pillow, Apply Pressure Against The Incision."Jhevilin RMNo ratings yet
- Gordon's Functional Health Pattern For Geriatric ClientsDocument8 pagesGordon's Functional Health Pattern For Geriatric ClientsGEN ERIGBUAGASNo ratings yet
- The Lawton Instrumental Activities of Daily Living ScaleDocument2 pagesThe Lawton Instrumental Activities of Daily Living ScaleGEN ERIGBUAGASNo ratings yet
- Katz Index of Independence in Activities of Daily LivingDocument1 pageKatz Index of Independence in Activities of Daily LivingGEN ERIGBUAGASNo ratings yet
- Nursing Care Plan Sample 7Document17 pagesNursing Care Plan Sample 7GEN ERIGBUAGASNo ratings yet
- Geriatric Functional AssessmentDocument5 pagesGeriatric Functional AssessmentGEN ERIGBUAGASNo ratings yet
- Nursing Care Plan Sample 5Document13 pagesNursing Care Plan Sample 5GEN ERIGBUAGASNo ratings yet
- Nursing Care Plan Sample 6Document17 pagesNursing Care Plan Sample 6GEN ERIGBUAGASNo ratings yet
- Principles of Long-Term Care and Palliative CareDocument3 pagesPrinciples of Long-Term Care and Palliative CareGEN ERIGBUAGASNo ratings yet
- Nursing Care Plan Sample 2Document9 pagesNursing Care Plan Sample 2GEN ERIGBUAGASNo ratings yet
- Health Assessment PortfolioDocument25 pagesHealth Assessment PortfolioGEN ERIGBUAGASNo ratings yet
- Emphysema - Pleurisy - Pleural EffusionDocument17 pagesEmphysema - Pleurisy - Pleural EffusionGEN ERIGBUAGASNo ratings yet
- Safety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/UndertakingDocument11 pagesSafety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/UndertakingjoseNo ratings yet
- SDS EN - Cambrex S31Document4 pagesSDS EN - Cambrex S31Dhruvi KansaraNo ratings yet
- Essentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full ChapterDocument67 pagesEssentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full Chapterhelen.fico427100% (4)
- c4 Raffinate 1 Etbe Ver 5 0 enDocument8 pagesc4 Raffinate 1 Etbe Ver 5 0 enLudi D. LunarNo ratings yet
- Bronchial Cancer Case StudyDocument3 pagesBronchial Cancer Case StudyericaNo ratings yet
- Scaffix Si-270 MsdsDocument6 pagesScaffix Si-270 Msdstaufiq hidayatNo ratings yet
- Pico INTLDocument180 pagesPico INTLAitorNo ratings yet
- Saturn Evo Color FolletoDocument2 pagesSaturn Evo Color FolletoEva TelloNo ratings yet
- Makalah B. Inggris SputumDocument8 pagesMakalah B. Inggris SputumDian FaqihNo ratings yet
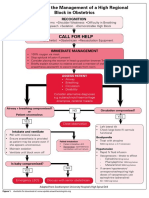
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- NozeSeal, LLC, Invention Helps Sleep Apnea PatientsDocument2 pagesNozeSeal, LLC, Invention Helps Sleep Apnea PatientsPR.comNo ratings yet
- 006 1048 0030 - Thinner 1048 MSDS PDFDocument9 pages006 1048 0030 - Thinner 1048 MSDS PDFBradyNo ratings yet
- Postural DrainageDocument6 pagesPostural DrainageKit Alizon Barredo0% (1)
- Cordillera Career Development College Buyagan, Poblacion, La Trinidad, Benguet Tel./Fax. No. (074) 422-2221/e-Mail Address: CCDC@CCDC - Edu.phDocument2 pagesCordillera Career Development College Buyagan, Poblacion, La Trinidad, Benguet Tel./Fax. No. (074) 422-2221/e-Mail Address: CCDC@CCDC - Edu.phleiNo ratings yet
- Material Safety Data Sheet: COMPLIES WITH 29 CFR 1910.1200. Osha Hazard Communication RuleDocument3 pagesMaterial Safety Data Sheet: COMPLIES WITH 29 CFR 1910.1200. Osha Hazard Communication Ruleeti apriyantiNo ratings yet
- Pediatric History Taking & Pe Simulation: Student'S Task Done Not DoneDocument8 pagesPediatric History Taking & Pe Simulation: Student'S Task Done Not DoneFrancis CervantesNo ratings yet
- F3 Chapter 1 (SOALAN) - RespirationDocument2 pagesF3 Chapter 1 (SOALAN) - Respirationleong cheng liyNo ratings yet
- Sulfuric Acid, 96% W/W: Safety Data SheetDocument8 pagesSulfuric Acid, 96% W/W: Safety Data SheetLindi PraditaNo ratings yet
- Impaired Skin Integrity Related To Excess Fluids Volume As Evidenced by Swelling of The Lower ExtremitiesDocument2 pagesImpaired Skin Integrity Related To Excess Fluids Volume As Evidenced by Swelling of The Lower ExtremitiesLevin MenpinNo ratings yet
- ACLS Protocols Pocket VersionDocument2 pagesACLS Protocols Pocket Versionjohndoe1995No ratings yet
- Normal and Abnormal Findings of Thorax and LungsDocument3 pagesNormal and Abnormal Findings of Thorax and LungsOtherin Ojibwa TejanoNo ratings yet
- Hands On CPR WorksheetDocument1 pageHands On CPR Worksheetapi-404833978No ratings yet
- MEDUMAT Transport 83428-ENDocument16 pagesMEDUMAT Transport 83428-ENShota MukhashavriaNo ratings yet
- CPR PosterDocument1 pageCPR PosterKent Joe AltarejosNo ratings yet
- Sds Calcium NitrateDocument5 pagesSds Calcium NitrateQuy NguyenNo ratings yet
- Compiled Skills LabDocument14 pagesCompiled Skills LabJolaine ValloNo ratings yet