You might also like
- Antifungal DrugsDocument45 pagesAntifungal DrugsAbdulai WakoNo ratings yet
- Anti-Fungal Agents: Jagir R. Patel Asst Professor Dept. PharmacologyDocument62 pagesAnti-Fungal Agents: Jagir R. Patel Asst Professor Dept. PharmacologyJagirNo ratings yet
- Antiprotozoal and AntihelminticDocument36 pagesAntiprotozoal and AntihelminticDiriba feyisaNo ratings yet
- Anti Fungal: Dr. Dr. Nico L Lumbuun, SPFKDocument45 pagesAnti Fungal: Dr. Dr. Nico L Lumbuun, SPFKAudhrey BNo ratings yet
- Antifungals: DR John TiongDocument58 pagesAntifungals: DR John TiongJia YingNo ratings yet
- Antifungal DrugsDocument20 pagesAntifungal DrugsboeykhNo ratings yet
- Anti Cancer ChemotherapyDocument103 pagesAnti Cancer ChemotherapyMourian AmanNo ratings yet
- ANTIFUNGAL AGENTS FOR FUNGAL INFECTIONSDocument24 pagesANTIFUNGAL AGENTS FOR FUNGAL INFECTIONSBaiqLinaAnggrianNo ratings yet
- ANTIFUNGAL AGENTS: A REVIEWDocument24 pagesANTIFUNGAL AGENTS: A REVIEWfitri dwiyantiNo ratings yet
- Antifungal Drugs: - Polyene Antibiotics: Amphotericin B, Nystatin - Antimetabolites: 5-Fluorocytosine - AzolesDocument18 pagesAntifungal Drugs: - Polyene Antibiotics: Amphotericin B, Nystatin - Antimetabolites: 5-Fluorocytosine - AzolesgopscharanNo ratings yet
- Immunomodulator 2014Document56 pagesImmunomodulator 2014LeilybadryaNo ratings yet
- Anti-Protozoal Drugs: Dr. Mozna TalpurDocument25 pagesAnti-Protozoal Drugs: Dr. Mozna TalpurShahid Hameed100% (1)
- Antifungal Classification and Mechanisms of ActionDocument55 pagesAntifungal Classification and Mechanisms of ActionAssssssNo ratings yet
- Antifungal Agents: Dewi Selvina R & Instiaty Department of Pharmacology FmuiDocument37 pagesAntifungal Agents: Dewi Selvina R & Instiaty Department of Pharmacology Fmuisalsa2506No ratings yet
- Drugs For Cancer TherapyDocument102 pagesDrugs For Cancer TherapyPUTRI CHRISTIANTI TELAUMBANUA 1No ratings yet
- Cancer Chemotherapy: A Guide to Pharmacology and Treatment StrategiesDocument51 pagesCancer Chemotherapy: A Guide to Pharmacology and Treatment StrategiesmaryamNo ratings yet
- AntiNeo SEDocument93 pagesAntiNeo SEJerome BentleyNo ratings yet
- Antifungal Drugs 1 (18Document46 pagesAntifungal Drugs 1 (18Elvis obajeNo ratings yet
- Anti-Fungal Drugs SushDocument31 pagesAnti-Fungal Drugs SushCheng XinvennNo ratings yet
- Antimycotic Agents and Their Properties: BY Mawuli AtiemoDocument25 pagesAntimycotic Agents and Their Properties: BY Mawuli AtiemoMawuli AtiemoNo ratings yet
- Antineoplastic DrugsDocument83 pagesAntineoplastic DrugsАббасси МокаммедNo ratings yet
- Anti-Tuberculosis Drugs Assignment 2024Document43 pagesAnti-Tuberculosis Drugs Assignment 2024Cleophas Nyangaresi100% (1)
- Revized 5 - Antifungal Medications - 2021Document28 pagesRevized 5 - Antifungal Medications - 2021احمد علىNo ratings yet
- 21 Anti-NeoplasticDocument11 pages21 Anti-NeoplasticMuhammad Amin BozdarNo ratings yet
- Antimalarial, Antiprotozoal, and Antihelmintic AgentsDocument37 pagesAntimalarial, Antiprotozoal, and Antihelmintic AgentsQuolette ConstanteNo ratings yet
- Properties and Mechanisms of Common AntibioticsDocument37 pagesProperties and Mechanisms of Common AntibioticsHa LeemNo ratings yet
- 15 Antifungal Drugs-Notes-3Document43 pages15 Antifungal Drugs-Notes-3Sindhu BabuNo ratings yet
- General Aspects of AntimicrobialsDocument62 pagesGeneral Aspects of AntimicrobialsShree pharmacy 10th batchNo ratings yet
- Anticancer Drugs Final PDFDocument8 pagesAnticancer Drugs Final PDFAisha Jamil100% (1)
- Pharmacology Antifungals Antithelminics Antimalarial DrugsDocument98 pagesPharmacology Antifungals Antithelminics Antimalarial DrugsAntonyNo ratings yet
- Cancer ChemotherapyDocument103 pagesCancer ChemotherapyTrang MaiNo ratings yet
- Antimycotic Agents and Their Properties: BY Mawuli Atiemo Central University College, AccraDocument25 pagesAntimycotic Agents and Their Properties: BY Mawuli Atiemo Central University College, AccraMawuli AtiemoNo ratings yet
- Antifungal AgentsDocument25 pagesAntifungal AgentsCham MontimanNo ratings yet
- Immunomodulators: Ma. Stephanie Fay S. Cagayan, MDDocument67 pagesImmunomodulators: Ma. Stephanie Fay S. Cagayan, MDFaye Cagayan100% (1)
- K12 - Pharmacology of Anticancer-NEW-1Document114 pagesK12 - Pharmacology of Anticancer-NEW-1Josephine IrenaNo ratings yet
- 9 - Anti Fungal DrugsDocument73 pages9 - Anti Fungal DrugsIjaz KhanNo ratings yet
- Antifungal AgentsDocument72 pagesAntifungal AgentsChristine OnyangoNo ratings yet
- Anthelmintic DrugDocument39 pagesAnthelmintic DrugBolanle OjokohNo ratings yet
- Antineoplastic Agents: Samuel A. Camorongan, RNDocument45 pagesAntineoplastic Agents: Samuel A. Camorongan, RNSamuel CamoronganNo ratings yet
- Lec 7 - AntibioticsDocument46 pagesLec 7 - AntibioticsAiqa QaziNo ratings yet
- Antifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Document37 pagesAntifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Hafsat JimetaNo ratings yet
- Cancer ChemotherapyDocument28 pagesCancer ChemotherapyFidelis LovelyNo ratings yet
- Antifungal Agents: Laboratorium Farmakologi Dan Terapi Fakultas Kedokteran Universitas Jenderal SoedirmanDocument51 pagesAntifungal Agents: Laboratorium Farmakologi Dan Terapi Fakultas Kedokteran Universitas Jenderal SoedirmanprofNo ratings yet
- Immuno Modulator SDocument62 pagesImmuno Modulator SAntony Prakash RajNo ratings yet
- Anticancer Drugs: Mechanisms and Side EffectsDocument13 pagesAnticancer Drugs: Mechanisms and Side EffectsPham PhamIoNo ratings yet
- EIGBEFOH Pharmacology of AntimicrobialsDocument59 pagesEIGBEFOH Pharmacology of AntimicrobialskbNo ratings yet
- Antifungal FDocument16 pagesAntifungal Fymeen9829No ratings yet
- Antifungal Drugs (Revised) Aug 2022Document62 pagesAntifungal Drugs (Revised) Aug 2022sankethNo ratings yet
- AminoglycosidesDocument20 pagesAminoglycosidesHassan.shehri100% (5)
- Antiprotozoal and AntihelminticDocument20 pagesAntiprotozoal and AntihelminticSami YGNo ratings yet
- Principles of Antimicrobial Therapy Part 1Document83 pagesPrinciples of Antimicrobial Therapy Part 1Carl Elexer Cuyugan Ano100% (1)
- Anti Fungal DrugsDocument18 pagesAnti Fungal DrugsAmrit paruaNo ratings yet
- S-Immunomodulator DrugsDocument48 pagesS-Immunomodulator DrugsFaishal100% (2)
- The Immunosuppression 2021Document10 pagesThe Immunosuppression 2021Muhammad AliNo ratings yet
- ERYTHROMYCINDocument22 pagesERYTHROMYCINhiraNo ratings yet
- Drugs For Neoplasia 2023Document24 pagesDrugs For Neoplasia 2023renz bartolomeNo ratings yet
- ANTINEOPLASTIC AGENTS AND THE CELL CYCLEDocument5 pagesANTINEOPLASTIC AGENTS AND THE CELL CYCLEKath DeguzmanNo ratings yet
- Anti FungalsDocument20 pagesAnti FungalsJUNKY DOCTORNo ratings yet
- Antifungal AgentsDocument22 pagesAntifungal AgentsQuolette Constante100% (1)
- Instapdf - in Pharmacology and Toxicology Mcqs With Answers 419 PDFDocument12 pagesInstapdf - in Pharmacology and Toxicology Mcqs With Answers 419 PDFDR AbidNo ratings yet
- INSAF CARD MEDICINE CHARGES Jun-19 to Dec-21Document1 pageINSAF CARD MEDICINE CHARGES Jun-19 to Dec-21DR AbidNo ratings yet
- Pharmacy Store Room Audit Finds Expired and Near Expiry MedicinesDocument1 pagePharmacy Store Room Audit Finds Expired and Near Expiry MedicinesDR AbidNo ratings yet
- COVID-19 VACCINE MISCONCEPTIONSDocument4 pagesCOVID-19 VACCINE MISCONCEPTIONSDR AbidNo ratings yet
- Update BillDocument1 pageUpdate BillDR AbidNo ratings yet
- MCQs in Pharmacology (PDFDrive)Document248 pagesMCQs in Pharmacology (PDFDrive)DR AbidNo ratings yet
- Available Medicine at PharmacyDocument4 pagesAvailable Medicine at PharmacyDR AbidNo ratings yet
- SodapdfDocument5 pagesSodapdfDR AbidNo ratings yet
- Pre Anesthetics Local AnestheticsDocument45 pagesPre Anesthetics Local AnestheticsDR AbidNo ratings yet
- Camp Patient DetailDocument2 pagesCamp Patient DetailDR AbidNo ratings yet
- Corticosteroid Drugs Uses and Side EffectsDocument5 pagesCorticosteroid Drugs Uses and Side EffectsDR AbidNo ratings yet
- Anti HypertensiveDocument4 pagesAnti HypertensiveDR AbidNo ratings yet
- Camp Patient DetailDocument2 pagesCamp Patient DetailDR AbidNo ratings yet
- Surgical PT Data 22Document4 pagesSurgical PT Data 22DR AbidNo ratings yet
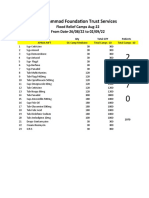
- Muhammad Foundation Flood Relief Camp Medicine ListDocument1 pageMuhammad Foundation Flood Relief Camp Medicine ListDR AbidNo ratings yet
- No of Patient Admitted Yearly Report of Packages in Gynae WardDocument1 pageNo of Patient Admitted Yearly Report of Packages in Gynae WardDR AbidNo ratings yet
- Emergency KITS MedicineDocument3 pagesEmergency KITS MedicineDR AbidNo ratings yet
- MCQ Points of PharmacologyDocument12 pagesMCQ Points of PharmacologyDR AbidNo ratings yet
- Camp Medicine Services Jan-22 to Dec-22Document8 pagesCamp Medicine Services Jan-22 to Dec-22DR AbidNo ratings yet
- Items Kept Temp Below 25Document1 pageItems Kept Temp Below 25DR AbidNo ratings yet
- Potassium SparingDocument22 pagesPotassium SparingDR AbidNo ratings yet
- 3rdyear Mbbs-Pharma Assignments-28th Week ResultDocument4 pages3rdyear Mbbs-Pharma Assignments-28th Week ResultDR AbidNo ratings yet
- 1st & 2nd Year Mbbs Teacher Report-22Document3 pages1st & 2nd Year Mbbs Teacher Report-22DR AbidNo ratings yet
- Tramadol Free of Cast FOR Every PatientDocument1 pageTramadol Free of Cast FOR Every PatientDR AbidNo ratings yet
- SodapdfDocument14 pagesSodapdfDR AbidNo ratings yet
- Insaf Card Medicine Record Jan-22 To July-22Document14 pagesInsaf Card Medicine Record Jan-22 To July-22DR AbidNo ratings yet
- Camp Daily SheetDocument688 pagesCamp Daily SheetDR AbidNo ratings yet
- Regarding Β Blockers: Liaquat University Of Medical & Health Sciences JamshoroDocument2 pagesRegarding Β Blockers: Liaquat University Of Medical & Health Sciences JamshoroDR AbidNo ratings yet
- PG Full OseDocument2 pagesPG Full OseDR AbidNo ratings yet
- NMJ Full OspeDocument2 pagesNMJ Full OspeDR AbidNo ratings yet
- Gender Essay Outline Eng102Document3 pagesGender Essay Outline Eng102Ella BobsNo ratings yet
- T e 2552674 Percy Polls Peculiar Plants Fiction Year 5 Reading Comprehension - Ver - 5Document20 pagesT e 2552674 Percy Polls Peculiar Plants Fiction Year 5 Reading Comprehension - Ver - 5mariam osamaNo ratings yet
- Business PolicyDocument17 pagesBusiness PolicyManish SinghNo ratings yet
- CAPS LESSON PLAN, KAHOOT QUIZ, PPT VIDEODocument3 pagesCAPS LESSON PLAN, KAHOOT QUIZ, PPT VIDEOMandisa MselekuNo ratings yet
- Serv Manual SM 100 FREEDocument75 pagesServ Manual SM 100 FREEGustavo Vargas Ruiz100% (1)
- Quantitative Data Analysis 2Document10 pagesQuantitative Data Analysis 2Rhona MaandalNo ratings yet
- Video Conferencing Lesson PlanDocument6 pagesVideo Conferencing Lesson PlanANN JILLIAN JOYCE MONDONEDO100% (1)
- Prob StatDocument1 pageProb StatSerenity VertesNo ratings yet
- Analysis of Security Issues in Web Applications Through Penetration TestingDocument7 pagesAnalysis of Security Issues in Web Applications Through Penetration Testingabdel_lakNo ratings yet
- An Implementation of Illuminance Meter Using Light Dependent Resistor Integrated With Labview ProgramDocument11 pagesAn Implementation of Illuminance Meter Using Light Dependent Resistor Integrated With Labview ProgramAshraf YusofNo ratings yet
- Akuntansi Keuangan Lanjutan - Akuntansi Penggabungan UsahaDocument67 pagesAkuntansi Keuangan Lanjutan - Akuntansi Penggabungan UsahachendyNo ratings yet
- WEG Low Voltage Motor Control Center ccm03 50044030 Brochure English PDFDocument12 pagesWEG Low Voltage Motor Control Center ccm03 50044030 Brochure English PDFRitaban222No ratings yet
- SRV210 - 250TC Spare PartsDocument2 pagesSRV210 - 250TC Spare PartsEnzo SovittiNo ratings yet
- Apparent Dip PDFDocument2 pagesApparent Dip PDFanon_114803412No ratings yet
- DEME Offshore Brochure_2022Document16 pagesDEME Offshore Brochure_2022amin32No ratings yet
- Orphanage Cum Old Age Home: Amruta Prakash BedmuthaDocument2 pagesOrphanage Cum Old Age Home: Amruta Prakash BedmuthaNamrata Bhandari100% (1)
- Diagnosing and Managing Acute and Chronic SinusitisDocument14 pagesDiagnosing and Managing Acute and Chronic SinusitisAnonymous y3TIOwX8100% (1)
- Studentwise Final Placement DetailsLast 3 YearsDocument18 pagesStudentwise Final Placement DetailsLast 3 YearsAmitNo ratings yet
- Exercise 1: Chọn đáp án đúng:: Buổi 9: Động từ khuyết thiếu (Modal verb)Document6 pagesExercise 1: Chọn đáp án đúng:: Buổi 9: Động từ khuyết thiếu (Modal verb)Huyền HồNo ratings yet
- Probability Tree Diagrams Solutions Mathsupgrade Co UkDocument10 pagesProbability Tree Diagrams Solutions Mathsupgrade Co UknatsNo ratings yet
- Duane Grant, A099 743 627 (BIA Sept. 9, 2016)Document12 pagesDuane Grant, A099 743 627 (BIA Sept. 9, 2016)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- RD218 Gardan 3110 Ob2226657 NDocument1 pageRD218 Gardan 3110 Ob2226657 Nopen hartigNo ratings yet
- V200 User ManualDocument171 pagesV200 User ManualuriahskyNo ratings yet
- IJPC 13 4 Hormone Replacement TherapyDocument92 pagesIJPC 13 4 Hormone Replacement TherapyMatiasNo ratings yet
- Smart Panels - Digitized Switchboards - Blokset Desing and Assembly GuideDocument94 pagesSmart Panels - Digitized Switchboards - Blokset Desing and Assembly Guidelorentz franklinNo ratings yet
- MJP Rate Schedule for Water Supply Pipeline ProjectDocument6 pagesMJP Rate Schedule for Water Supply Pipeline ProjectJalal TamboliNo ratings yet
- LC1D150M7: Product Data SheetDocument3 pagesLC1D150M7: Product Data SheetTrong Hung NguyenNo ratings yet
- Sax AltoDocument2 pagesSax AltoJohnny GervasioNo ratings yet
- Main Body Recruitment Process of Human Resource Division in Brac BankDocument55 pagesMain Body Recruitment Process of Human Resource Division in Brac BankAsfia PrantyNo ratings yet
- SP Manual Addendum For OS 3 - 03Document2 pagesSP Manual Addendum For OS 3 - 03kevmac88No ratings yet