You might also like
- It 4 - Sel Dan Jaringan Sistim ImunDocument90 pagesIt 4 - Sel Dan Jaringan Sistim Imunezra soNo ratings yet
- Basic Immunology Final Edit2Document158 pagesBasic Immunology Final Edit2chippaiqweqweNo ratings yet
- Immune Response: Cell Biology and Its Application BI-1202Document35 pagesImmune Response: Cell Biology and Its Application BI-1202Eriani Wulandari100% (1)
- DR - Gold Immunology NotesDocument11 pagesDR - Gold Immunology NotesAaron PhuaNo ratings yet
- Introduction Immune System S2 DD 2020Document84 pagesIntroduction Immune System S2 DD 2020Belia Bima NafisaNo ratings yet
- The Immune System: Back To The BasicsDocument37 pagesThe Immune System: Back To The BasicsHani GowaiNo ratings yet
- Immnunology Notebook Chapter One: Innate ImmunityDocument45 pagesImmnunology Notebook Chapter One: Innate ImmunityJavier Alejandro Daza GalvánNo ratings yet
- Use action buttons to navigate tutorialDocument49 pagesUse action buttons to navigate tutorialleeNo ratings yet
- Introduction To ImmunologyDocument14 pagesIntroduction To Immunologykaiyeol exoNo ratings yet
- The Resistance Offered by The Host Towards Injury Caused by Microorganisms and Their Products or The State of Protection From Infectious DiseaseDocument21 pagesThe Resistance Offered by The Host Towards Injury Caused by Microorganisms and Their Products or The State of Protection From Infectious DiseaseReshmiAkhilNo ratings yet
- CytokinesDocument12 pagesCytokinesclventuriniNo ratings yet
- Basic Immunology 2Document66 pagesBasic Immunology 2JabbarTapiheruNo ratings yet
- Lymphocytes T-Cells & B-Cells: Urmia University Supervisor: Dr. NajafiDocument59 pagesLymphocytes T-Cells & B-Cells: Urmia University Supervisor: Dr. NajafiMh BzNo ratings yet
- Lecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesDocument70 pagesLecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesJoe JoeNo ratings yet
- Esi (1Document114 pagesEsi (1Ferina Mega SilviaNo ratings yet
- Cell-Mediated Immune Responses8Document26 pagesCell-Mediated Immune Responses8Trifu AndreiNo ratings yet
- The Colonic Phase of The Integrated Response To A MealDocument9 pagesThe Colonic Phase of The Integrated Response To A MealpuchioNo ratings yet
- LECTURE 1 HANDOUT Online ImmuneDocument28 pagesLECTURE 1 HANDOUT Online ImmuneFYMNo ratings yet
- Tissue and Organs of The Immune System: Learning GoalsDocument113 pagesTissue and Organs of The Immune System: Learning Goalsbright nvachirawit100% (1)
- Innate ImmunityDocument9 pagesInnate Immunitynascha dumpNo ratings yet
- Physiology L6Document6 pagesPhysiology L6Anonymous elq7jZiSNo ratings yet
- The Biology of Apoptosis: Fouad Boulos, MD August 2010Document4 pagesThe Biology of Apoptosis: Fouad Boulos, MD August 2010ans11No ratings yet
- Immune Disorders ExplainedDocument5 pagesImmune Disorders ExplainedThalia Fortune100% (1)
- Embryology Reviewer Chapter 1 and 2Document9 pagesEmbryology Reviewer Chapter 1 and 2Allison Eunice ServandoNo ratings yet
- Integrated Lecture - Innate Immune Response (2022)Document56 pagesIntegrated Lecture - Innate Immune Response (2022)Nabilah DENo ratings yet
- Concept On Immune Response and Inflammation REVISEDDocument163 pagesConcept On Immune Response and Inflammation REVISEDKirk08100% (1)
- Humoral & Celullar ImmunityDocument60 pagesHumoral & Celullar ImmunityHaziq KamardinNo ratings yet
- Embryo NotesDocument52 pagesEmbryo NotesSharona Avgush100% (1)
- Comparing Primary and Secondary Immune ResponsesDocument3 pagesComparing Primary and Secondary Immune ResponsesMarta DaNo ratings yet
- Human MicrobiomeDocument13 pagesHuman MicrobiomeHabab Ali AhmadNo ratings yet
- M T Ch16 Innate Immunity SDocument30 pagesM T Ch16 Innate Immunity SAnonymous STRYVGKNo ratings yet
- 1 Juliane Flores Bible FinalDocument170 pages1 Juliane Flores Bible FinalJuliane FloresNo ratings yet
- Bio Mechanics Lecture NotesDocument53 pagesBio Mechanics Lecture NotesscdubalNo ratings yet
- Cytokines 2Document102 pagesCytokines 2api-273068056No ratings yet
- Gland Hormone Function Target Organ (Name or Picture) : HypothalamusDocument2 pagesGland Hormone Function Target Organ (Name or Picture) : HypothalamusRoya ImaniNo ratings yet
- Anti-Microbial Therapy Final With AlarmsDocument245 pagesAnti-Microbial Therapy Final With AlarmsMahmoud Ahmed MahmoudNo ratings yet
- Introduction To Endocrinology For Clinical StudentsDocument28 pagesIntroduction To Endocrinology For Clinical StudentsOhwovoriole ToketemuNo ratings yet
- 12 Edition of International Conference On Microbiology, Antibiotics and Public HealthDocument6 pages12 Edition of International Conference On Microbiology, Antibiotics and Public HealthMicrobiology MicrobiologyNo ratings yet
- Cell Signaling in Space and Time:: Where Proteins Come Together and When They're ApartDocument20 pagesCell Signaling in Space and Time:: Where Proteins Come Together and When They're ApartHumbertoNo ratings yet
- Pharm Exam Ii NotesDocument24 pagesPharm Exam Ii Noteskatiana louisNo ratings yet
- Organs of The Immune SystemDocument19 pagesOrgans of The Immune SystemprabuNo ratings yet
- Endocrine System: By: Trixie Rose E. CortezDocument144 pagesEndocrine System: By: Trixie Rose E. CortezTrixie Rose Ebona CortezNo ratings yet
- Big Question: What Happens When Immune System Overreacts?Document42 pagesBig Question: What Happens When Immune System Overreacts?Louloun MoussignacNo ratings yet
- B Cell PDFDocument65 pagesB Cell PDFChandan KumarNo ratings yet
- Unit 13 Endocrine GlandDocument73 pagesUnit 13 Endocrine GlandChandan ShahNo ratings yet
- Gallbladder & Bile Physiological AspectsDocument48 pagesGallbladder & Bile Physiological AspectsPhysiology by Dr RaghuveerNo ratings yet
- Handouts Immune Defenses F11Document12 pagesHandouts Immune Defenses F11Kelly Trainor100% (1)
- 10 Muscular ContractionDocument29 pages10 Muscular ContractionMark Piedad MillanoNo ratings yet
- The Immune SystemDocument15 pagesThe Immune SystemAslak Torgersen100% (1)
- NERVOUS PhysiologyDocument85 pagesNERVOUS PhysiologyHenok GirmaNo ratings yet
- Summary Table Endocrine Review - OneDocument5 pagesSummary Table Endocrine Review - OneIndigoSilverNo ratings yet
- Basic Immunology: An Overview of the Immune System and Its FunctionsDocument101 pagesBasic Immunology: An Overview of the Immune System and Its FunctionsZas VutraNo ratings yet
- MHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsDocument25 pagesMHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsMudassar Roomi100% (1)
- Bacterial PathogenesisDocument36 pagesBacterial Pathogenesisapi-19969058100% (3)
- 16/09/2015 1 Mujtaba AshrafDocument44 pages16/09/2015 1 Mujtaba Ashrafதீரன் சக்திவேல்No ratings yet
- Key Concepts of EndocrinologyDocument131 pagesKey Concepts of Endocrinologykomal pattabiNo ratings yet
- Apoptosis and CaspasesDocument19 pagesApoptosis and CaspasesKunhutty Vasudevan AnubhamaNo ratings yet
- Companion Diagnostics or Theranostics Products in The MarketDocument3 pagesCompanion Diagnostics or Theranostics Products in The MarkettonnymjohnsonNo ratings yet
- UNIT 1 ImmunologyDocument82 pagesUNIT 1 ImmunologySivarama KrishnanNo ratings yet
- Immunity 2022Document53 pagesImmunity 2022Craft Hachz By dhiyaNo ratings yet
- Avicel 105 COADocument1 pageAvicel 105 COAAshish ChangediyaNo ratings yet
- Avicel 105 COADocument1 pageAvicel 105 COAAshish ChangediyaNo ratings yet
- Scanned With CamscannerDocument19 pagesScanned With CamscannerAshish ChangediyaNo ratings yet
- Working Women's Rights For Maternity BenefitsDocument4 pagesWorking Women's Rights For Maternity BenefitsAshish ChangediyaNo ratings yet
- Workman's Right To Compensation For Accidents and Occupational DiseasesDocument11 pagesWorkman's Right To Compensation For Accidents and Occupational DiseasesAshish ChangediyaNo ratings yet
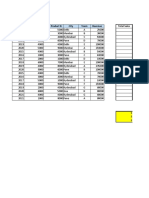
- Excel - Assignment - 1 (1Document16 pagesExcel - Assignment - 1 (1Ashish ChangediyaNo ratings yet
- Immunology and Immuno BiotechnologyDocument45 pagesImmunology and Immuno BiotechnologySaravanan RajagopalNo ratings yet
- Characteristics of the Complement SystemDocument51 pagesCharacteristics of the Complement SystemFrancisco NiegasNo ratings yet
- Physiology ImmunityDocument75 pagesPhysiology Immunitymohani maiyaNo ratings yet
- Tema 3 - Inmune Responses To ImplantsDocument18 pagesTema 3 - Inmune Responses To ImplantsIsrael GonzálezNo ratings yet
- The 20-character complement system overviewDocument32 pagesThe 20-character complement system overviewMona AdamNo ratings yet
- Turgeon Review QuestionsDocument88 pagesTurgeon Review QuestionsMedTech FilesNo ratings yet
- Biomedis ImunsistemDocument49 pagesBiomedis ImunsistemDede MulyamanNo ratings yet
- Mind Map TonsillitisDocument1 pageMind Map TonsillitisKubraNo ratings yet
- Microbial Interactions With The Host in Periodontal DiseasesDocument74 pagesMicrobial Interactions With The Host in Periodontal Diseasesrupali100% (2)
- The Complement System: A Cascade Defense Against MicrobesDocument27 pagesThe Complement System: A Cascade Defense Against MicrobesSai Kiran100% (1)
- Complement System: Cascade, Is A Part of The Immune System That EnhancesDocument10 pagesComplement System: Cascade, Is A Part of The Immune System That Enhancesfelipe smithNo ratings yet
- Immunology 2Document50 pagesImmunology 2niripsaNo ratings yet
- Stevens Immuno Sero Answer KeyDocument18 pagesStevens Immuno Sero Answer KeyKATHERINE SHYLE MILARNo ratings yet
- Janeway Chapter Question AnswersDocument9 pagesJaneway Chapter Question AnswersNguyễn Nam AnhNo ratings yet
- Complement-System Complement - SystemDocument6 pagesComplement-System Complement - Systemrenato renatoNo ratings yet
- Refresh: PathologyDocument160 pagesRefresh: PathologyManasa Addala100% (1)
- Molecular Immunology: Claire L. Harris, Richard B. Pouw, David Kavanagh, Ruyue Sun, Daniel RicklinDocument31 pagesMolecular Immunology: Claire L. Harris, Richard B. Pouw, David Kavanagh, Ruyue Sun, Daniel Ricklinguugle gogleNo ratings yet
- Chapter 15 Innate ImmunityDocument38 pagesChapter 15 Innate Immunityapi-270625839No ratings yet
- Complement System: Zaahira Gani, Cambridge, UKDocument2 pagesComplement System: Zaahira Gani, Cambridge, UKShardendu PandeyNo ratings yet
- Complement SystemDocument4 pagesComplement SystemFait HeeNo ratings yet
- Full Download Test Bank For Janeways Immunobiology 9th Edition PDF Full ChapterDocument36 pagesFull Download Test Bank For Janeways Immunobiology 9th Edition PDF Full Chaptersuckapyrexy.pe70th100% (18)
- Path NotesDocument255 pagesPath NotesEvangeline MaryNo ratings yet
- ImmunoDocument18 pagesImmunoirish o-oNo ratings yet
- Refresh Pathology 3rd Ed. 2022-Dr. Shiva MDDocument220 pagesRefresh Pathology 3rd Ed. 2022-Dr. Shiva MD147-haricharan voduri100% (1)
- Immunology and Serology NotesDocument171 pagesImmunology and Serology NotesMa Loidette Rull Guanlao-Serrano67% (3)
- Sentul Point June16 AgentDocument57 pagesSentul Point June16 AgentNanthini PalanisamyNo ratings yet
- Acute Inflammation ExplainedDocument13 pagesAcute Inflammation ExplainedWilliam BufNo ratings yet
- Refresh Pathology 1Document179 pagesRefresh Pathology 1Syed IbraheemNo ratings yet
- Kuis Imun UTSDocument8 pagesKuis Imun UTSichiNo ratings yet
- Immunosero Notes 2Document20 pagesImmunosero Notes 2Rakim MikarNo ratings yet