You might also like
- Blood Pressure HomeostasisDocument7 pagesBlood Pressure HomeostasisHassan Al SinanNo ratings yet
- Blood Pressure RegulationDocument3 pagesBlood Pressure RegulationiMaibelle BelleNo ratings yet
- Blood Pressure AssignmentDocument19 pagesBlood Pressure AssignmentADITYAROOP PATHAKNo ratings yet
- Blood Pressure: By: Saiyed Falakaara Assistant Professor Department of Pharmacy Sumandeep VidyapeethDocument26 pagesBlood Pressure: By: Saiyed Falakaara Assistant Professor Department of Pharmacy Sumandeep VidyapeethFalak AaraNo ratings yet
- Blood Pressure RegulationDocument35 pagesBlood Pressure Regulationبراءة أحمد السلاماتNo ratings yet
- Heart Rate Blood PressureDocument128 pagesHeart Rate Blood PressureShubhra ShettyNo ratings yet
- Blood PressureDocument26 pagesBlood PressureEniola DaramolaNo ratings yet
- Blood PressureDocument8 pagesBlood PressureUmair RaoNo ratings yet
- Blood Pressure Regulation - 0Document19 pagesBlood Pressure Regulation - 0Ehtiram HuseynovNo ratings yet
- Blood PressureDocument58 pagesBlood PressureAyurveda PgNo ratings yet
- Blood LossDocument6 pagesBlood LossDungani AllanNo ratings yet
- II. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCDocument12 pagesII. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCapi-290338101No ratings yet
- Shock PresentaionDocument30 pagesShock PresentaionKennedy Ng'andweNo ratings yet
- Short-Term Regulation of Blood PressureDocument5 pagesShort-Term Regulation of Blood PressureRae OkonNo ratings yet
- Chapter 7 Regulation of Arterial Blood Pressure and MicrocirculationDocument20 pagesChapter 7 Regulation of Arterial Blood Pressure and Microcirculationaisyahasrii_No ratings yet
- Barorecceptori Și Controlul Presiunilor de SângeDocument3 pagesBarorecceptori Și Controlul Presiunilor de SângeAurelia AlexandraNo ratings yet
- CVS Regulation IIDocument33 pagesCVS Regulation IIbiradarbhagya773No ratings yet
- 25circulation Part 3Document15 pages25circulation Part 3Jaydave PatelNo ratings yet
- CVS Lect 6 Blood Pressure, PathophysiologyDocument13 pagesCVS Lect 6 Blood Pressure, PathophysiologySherwan R Shal100% (5)
- Physiological Regulation of Arterial Blood PressureDocument36 pagesPhysiological Regulation of Arterial Blood PressureFrancesNo ratings yet
- Arterial Pressure RegulationDocument50 pagesArterial Pressure RegulationareebNo ratings yet
- Reflex Control of The CirculationDocument7 pagesReflex Control of The CirculationAbigail ChristisnNo ratings yet
- Nervous Regulation of The Circulation and Rapid Control of Arterial PressureDocument2 pagesNervous Regulation of The Circulation and Rapid Control of Arterial Pressuremcwnotes100% (2)
- Blood Pressure SummaryDocument7 pagesBlood Pressure SummaryNancy You100% (1)
- Reduced BRS Can Indicate:: Scientific ServicesDocument1 pageReduced BRS Can Indicate:: Scientific ServicesJoko AsleyNo ratings yet
- Applied Cardiovascular PhysiologyDocument1 pageApplied Cardiovascular Physiologyoperation KDNANo ratings yet
- Regulation of Blood PressureDocument5 pagesRegulation of Blood PressureKing kakaNo ratings yet
- The Circulatory System in MammalsDocument29 pagesThe Circulatory System in MammalsKeanna RaphaelNo ratings yet
- Blood PressureDocument57 pagesBlood PressureMatende husseinNo ratings yet
- Baroreceptors and Therefore The Sympathetic SystemDocument5 pagesBaroreceptors and Therefore The Sympathetic SystemS GNo ratings yet
- Resumen CardioDocument15 pagesResumen CardioSofia LacuadraNo ratings yet
- Blood PressureDocument23 pagesBlood PressuresureshNo ratings yet
- The Circulatory System Group 2Document17 pagesThe Circulatory System Group 2sanique peterkinNo ratings yet
- Arterial Blood PressureDocument7 pagesArterial Blood Pressuredhoha alawsiNo ratings yet
- Blood Pressure Regulation HandoutDocument10 pagesBlood Pressure Regulation Handoutsac50900100% (2)
- מצגת4Document24 pagesמצגת4Rahaf MajadlyNo ratings yet
- Presion ArterialDocument26 pagesPresion ArterialAndrea SuazoNo ratings yet
- Blood Pressure RegulationDocument4 pagesBlood Pressure Regulationmutisya.mathuvaNo ratings yet
- My Lecture13 - Cardiovascular PhysiologyDocument16 pagesMy Lecture13 - Cardiovascular PhysiologyVivek ChaudharyNo ratings yet
- CVS 5Document6 pagesCVS 5MayankNo ratings yet
- GroupWorkSOLERANTOQUEPLAZA MCNSG3Document4 pagesGroupWorkSOLERANTOQUEPLAZA MCNSG3Leah AntoqueNo ratings yet
- Heart QuizDocument1 pageHeart QuizNaNo ratings yet
- Blood Pressure Regulation - SlidesDocument35 pagesBlood Pressure Regulation - Slidesمحمد السنجلاويNo ratings yet
- Long & Short Term Regulation of BPDocument50 pagesLong & Short Term Regulation of BPntambik21No ratings yet
- Homeostasis of The Cardiovascular SystemDocument7 pagesHomeostasis of The Cardiovascular SystemdesbestNo ratings yet
- .SHOCK, Alice - 1704638750000Document12 pages.SHOCK, Alice - 1704638750000Nakintu AliceNo ratings yet
- CV PathoDocument32 pagesCV PathoSaif AliNo ratings yet
- Humoral and Intra Cardiac Mechanism of Heart' RegulationDocument23 pagesHumoral and Intra Cardiac Mechanism of Heart' RegulationAman singhNo ratings yet
- CVS PharmacologyDocument19 pagesCVS Pharmacologymug ashNo ratings yet
- The Normal Physiology of The Heart: Vikkineshwaran Siva SubramaniamDocument4 pagesThe Normal Physiology of The Heart: Vikkineshwaran Siva SubramaniamSivamala MalaNo ratings yet
- Cardiac OutputDocument18 pagesCardiac OutputGauravSinghNo ratings yet
- Cardiovascular Physiology: The Autonomic Nervous SystemDocument8 pagesCardiovascular Physiology: The Autonomic Nervous SystemRidha Surya NugrahaNo ratings yet
- Hemodynamics For The Bedside Nurse 1CEUDocument7 pagesHemodynamics For The Bedside Nurse 1CEURN333100% (1)
- Case 2 SlosDocument7 pagesCase 2 SlosNamarNo ratings yet
- Chap+13+CoordinatedCVSFall11 1Document10 pagesChap+13+CoordinatedCVSFall11 1Drbee10No ratings yet
- Physiology of Blood PressureDocument4 pagesPhysiology of Blood PressureNoorNo ratings yet
- Abnormal Circulation: Heart Failure (Pump Energy Failure)Document6 pagesAbnormal Circulation: Heart Failure (Pump Energy Failure)Aga AquinoNo ratings yet
- Untitled NotebookDocument4 pagesUntitled NotebookMohamed HamzaNo ratings yet
- Blood Pressure-For StudentsDocument79 pagesBlood Pressure-For StudentsAshok Kumar P100% (1)
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Journal Pre-Proof: Clinics in DermatologyDocument17 pagesJournal Pre-Proof: Clinics in Dermatologymaat1No ratings yet
- Chapter 21 - Blood Vessels and CirculationDocument13 pagesChapter 21 - Blood Vessels and CirculationSameer AkhtarNo ratings yet
- Percubaan Biologi Kertas 1 Melaka 2016Document29 pagesPercubaan Biologi Kertas 1 Melaka 2016Siti Norliana JohariNo ratings yet
- Micro A, 7 Heart - BV'sDocument76 pagesMicro A, 7 Heart - BV'sVictoria TanNo ratings yet
- Pre EclampsiaDocument18 pagesPre EclampsiaMary BlancoNo ratings yet
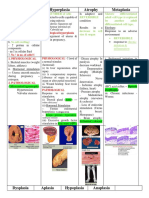
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- What Is Light?: Figure 1: Light Always Travels in Straight LineDocument16 pagesWhat Is Light?: Figure 1: Light Always Travels in Straight LineAjitNo ratings yet
- Workbook Answers PDFDocument36 pagesWorkbook Answers PDFPeriperi PeriperiNo ratings yet
- Using Wavelet Analysis To Characterize The Thermoregulatory Mechanisms of Sacral Skin Blood FlowDocument9 pagesUsing Wavelet Analysis To Characterize The Thermoregulatory Mechanisms of Sacral Skin Blood Flowh6j4vsNo ratings yet
- Grade 11 Science 2nd Term Test Paper 2019 English Medium - North Western ProvinceDocument23 pagesGrade 11 Science 2nd Term Test Paper 2019 English Medium - North Western ProvinceNethu NethuNo ratings yet
- Sindrom Multiple Disfungsi OrganDocument8 pagesSindrom Multiple Disfungsi OrganAdi Nugroho MelyanaNo ratings yet
- Prof. Mark Jheran Alvarez, USRN, MAN-MSDocument52 pagesProf. Mark Jheran Alvarez, USRN, MAN-MSMark Jheran AlvarezNo ratings yet
- DR John H Rundback Describes How Patients With Diabetic Can Prevent Peripheral Arterial Disease Ulceration and D?gradationirzth PDFDocument2 pagesDR John H Rundback Describes How Patients With Diabetic Can Prevent Peripheral Arterial Disease Ulceration and D?gradationirzth PDFJoyceJuel2No ratings yet
- NCM 106 - Week 2 (Cardiovascular P1) (Midterm)Document7 pagesNCM 106 - Week 2 (Cardiovascular P1) (Midterm)MARIA KAWILANNo ratings yet
- PMLS 2 PrelimsDocument55 pagesPMLS 2 PrelimsCassey Stephane PinedaNo ratings yet
- AIDA3 Pool Manual - EnglishDocument97 pagesAIDA3 Pool Manual - EnglishHimar Mendoza MárquezNo ratings yet
- CVS Lect 6 Blood Pressure, PathophysiologyDocument13 pagesCVS Lect 6 Blood Pressure, PathophysiologySherwan R Shal100% (5)
- PIH CASE FinalDocument35 pagesPIH CASE FinalrJ67% (3)
- Science: Quarter 2 - Module 2: The Human Body SystemsDocument32 pagesScience: Quarter 2 - Module 2: The Human Body SystemsJonel Buergo100% (9)
- Friday 8 January 2021: BiologyDocument28 pagesFriday 8 January 2021: BiologyhassanNo ratings yet
- Multiple Choice Questions (MCQ) Topic Quiz Cardiovascular SystemDocument19 pagesMultiple Choice Questions (MCQ) Topic Quiz Cardiovascular SystemMarimuthu ANo ratings yet
- TUNG Alex AcostaDocument74 pagesTUNG Alex AcostaJose Miguel Seguela Flores100% (2)
- FARRINGTON - Clinical Materia MedicaDocument408 pagesFARRINGTON - Clinical Materia MedicaMahmood Mufti100% (2)
- Biology 2 Chapter 4Document61 pagesBiology 2 Chapter 4Malas Nak TaipNo ratings yet
- What Keeps The Blood Moving!Document25 pagesWhat Keeps The Blood Moving!mikeeNo ratings yet
- Sci9 U1M1 LM v1.0Document27 pagesSci9 U1M1 LM v1.0catherinerenante50% (2)
- Forensic Medicine 1Document51 pagesForensic Medicine 1Whed Mark Rebudan IINo ratings yet
- Test I. Multiple Choice. Encircle The Letter of The Correct AnswerDocument6 pagesTest I. Multiple Choice. Encircle The Letter of The Correct AnswerDaisuke InoueNo ratings yet
- A Patient With Oedema PresentationDocument35 pagesA Patient With Oedema PresentationWasswaNo ratings yet
- Massage - Anatomy and Massage Course NotesDocument18 pagesMassage - Anatomy and Massage Course NotesMarcel FagadarNo ratings yet