You might also like
- BBD - Conference ProceedingsDocument10 pagesBBD - Conference ProceedingsTommy JohnsonNo ratings yet
- The Secretary/Principal Secretary: Can Be Placed With The Schemes Such As MGNREGS, PMAY, NSAP, Cte, As Per TheirDocument2 pagesThe Secretary/Principal Secretary: Can Be Placed With The Schemes Such As MGNREGS, PMAY, NSAP, Cte, As Per TheirTommy JohnsonNo ratings yet
- EXCRETIONDocument16 pagesEXCRETIONTommy JohnsonNo ratings yet
- Our Services Highways, Bridges & Traffic Division: Shree ConsultantsDocument4 pagesOur Services Highways, Bridges & Traffic Division: Shree ConsultantsTommy JohnsonNo ratings yet
- The Secretary/Principal Secretary: Can Be Placed With The Schemes Such As MGNREGS, PMAY, NSAP, Cte, As Per TheirDocument2 pagesThe Secretary/Principal Secretary: Can Be Placed With The Schemes Such As MGNREGS, PMAY, NSAP, Cte, As Per TheirTommy JohnsonNo ratings yet
- DISTRIBUTIONDocument7 pagesDISTRIBUTIONTommy JohnsonNo ratings yet
- Bulk DrugDocument19 pagesBulk DrugTommy JohnsonNo ratings yet
- Chemical ReactionDocument24 pagesChemical ReactionTommy JohnsonNo ratings yet
- Pharmaco DynamicsDocument11 pagesPharmaco DynamicsTommy JohnsonNo ratings yet
- Principles For Layout of Bulk Production Facilities: Green FieldDocument17 pagesPrinciples For Layout of Bulk Production Facilities: Green FieldTommy JohnsonNo ratings yet
- Biotechnology Based ProcessDocument26 pagesBiotechnology Based ProcessTommy JohnsonNo ratings yet
- METABOLISMDocument32 pagesMETABOLISMTommy JohnsonNo ratings yet
- Transposition of The Great Arteries (TGA)Document4 pagesTransposition of The Great Arteries (TGA)Tommy JohnsonNo ratings yet
- Principles For Layout of Bulk Production Facilities: Green FieldDocument17 pagesPrinciples For Layout of Bulk Production Facilities: Green FieldTommy JohnsonNo ratings yet
- Chemical ReactionDocument24 pagesChemical ReactionTommy JohnsonNo ratings yet
- Bulk DrugDocument19 pagesBulk DrugTommy JohnsonNo ratings yet
- Biotechnology Based ProcessDocument26 pagesBiotechnology Based ProcessTommy JohnsonNo ratings yet
- Meaning of AccountingDocument9 pagesMeaning of AccountingTommy JohnsonNo ratings yet
- Biopharmaceutical Industry: Biotechnology and Pharmaceutical IndustryDocument27 pagesBiopharmaceutical Industry: Biotechnology and Pharmaceutical IndustryTommy JohnsonNo ratings yet
- Experimental Study On Hollow Blocks With Wastes: ProceedingsDocument7 pagesExperimental Study On Hollow Blocks With Wastes: ProceedingsTommy JohnsonNo ratings yet
- Pharmaco DynamicsDocument11 pagesPharmaco DynamicsTommy JohnsonNo ratings yet
- Biogas Plant Based On Kitchen Waste: Nuclear Agriculture and Biotechnology DivisionDocument4 pagesBiogas Plant Based On Kitchen Waste: Nuclear Agriculture and Biotechnology Divisionabhin0582No ratings yet
- Data Science at WorkDocument14 pagesData Science at WorkTommy JohnsonNo ratings yet
- Is 456Document26 pagesIs 456Tommy JohnsonNo ratings yet
- Biogas Presentation R&D CellDocument9 pagesBiogas Presentation R&D CellTommy JohnsonNo ratings yet
- BBD - Conference ProceedingsDocument10 pagesBBD - Conference ProceedingsTommy JohnsonNo ratings yet
- Building DrawingDocument6 pagesBuilding DrawingTommy JohnsonNo ratings yet
- H21-Influence of Crude Source On The Viscous Properties of Blended Asphalt PDFDocument6 pagesH21-Influence of Crude Source On The Viscous Properties of Blended Asphalt PDFTommy JohnsonNo ratings yet
- Traffic Full BookDocument69 pagesTraffic Full BookTommy JohnsonNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Silica Sols and Colloidal Silica 2007Document4 pagesSilica Sols and Colloidal Silica 2007veroniqueNo ratings yet
- Histamine, Serotonin & The Ergot AlkaloidsDocument31 pagesHistamine, Serotonin & The Ergot AlkaloidsnicewanNo ratings yet
- Fumed or Pyrogenic Silica Global Market - Trends 2016-2018 and Forecast 2019-2025Document4 pagesFumed or Pyrogenic Silica Global Market - Trends 2016-2018 and Forecast 2019-2025Industry Experts, Inc.No ratings yet
- 2016 Bio Productions CatalogueDocument36 pages2016 Bio Productions Cataloguekaduwd100% (1)
- Vol.46-6 2028 PDFDocument10 pagesVol.46-6 2028 PDFShelly-zaKhwairakpamNo ratings yet
- 4th QUARTEST TEST SCIENCE 7Document6 pages4th QUARTEST TEST SCIENCE 7Geraldine Dioquino RosalesNo ratings yet
- A-Level Chemistry SyllabusDocument61 pagesA-Level Chemistry SyllabusLabiba GulNo ratings yet
- Ip143 Asphaltenes (Heptane Insolubles)Document7 pagesIp143 Asphaltenes (Heptane Insolubles)muhammad isaNo ratings yet
- HUBS1403 - Biomedical Science 1 - Lecture 4. Carbohydrates and LipidsDocument33 pagesHUBS1403 - Biomedical Science 1 - Lecture 4. Carbohydrates and LipidsEvelyn YongNo ratings yet
- F0503HDocument12 pagesF0503HSopon SrirattanapiboonNo ratings yet
- Bun PT Introducere - Removal of Cytostatic Drugs From Aquatic Environment A ReviewDocument18 pagesBun PT Introducere - Removal of Cytostatic Drugs From Aquatic Environment A ReviewsorinamotocNo ratings yet
- Avocado Seed Extract AnalysisDocument14 pagesAvocado Seed Extract AnalysisRatna SariNo ratings yet
- MSDS Hydraulic-Hydrostatic Fluid ExxonMobilDocument10 pagesMSDS Hydraulic-Hydrostatic Fluid ExxonMobilMaria Angelica Gomez PintoNo ratings yet
- 4 Types of Engineering Materials & Their CategoriesDocument3 pages4 Types of Engineering Materials & Their Categoriesiyouezra100% (4)
- Water Soluble Polymer Flocculants Synthesis, PDFDocument43 pagesWater Soluble Polymer Flocculants Synthesis, PDFruizgj2011No ratings yet
- Plastic Roads (Ang)Document17 pagesPlastic Roads (Ang)Feryani DoniaNo ratings yet
- Low cost micropropagation of bananaDocument14 pagesLow cost micropropagation of bananaHabibullah KhanNo ratings yet
- CHE026L Lab Activity Sheet #5: Ionic and Covalent BondsDocument7 pagesCHE026L Lab Activity Sheet #5: Ionic and Covalent BondsZeian Jacob BaylaNo ratings yet
- Mammalian Toxicology of Cetrimonium Chloride: Applicable To These Current Stepan ProductsDocument3 pagesMammalian Toxicology of Cetrimonium Chloride: Applicable To These Current Stepan Productsmohamed AdelNo ratings yet
- Cable Pulling Lubricant - Data Sheet (En Ingles)Document2 pagesCable Pulling Lubricant - Data Sheet (En Ingles)angel de mi guardaNo ratings yet
- Industrial ToxicologyDocument2 pagesIndustrial ToxicologyHadiaNo ratings yet
- Msds Nitrogen DioxideDocument8 pagesMsds Nitrogen DioxideBudiSetiawanNo ratings yet
- ALA Ver. 3.2Document37 pagesALA Ver. 3.2Yoga SunardiNo ratings yet
- Research Article Role of EnzymesDocument3 pagesResearch Article Role of Enzymesdwi pambuko anantiNo ratings yet
- DHANRAJDocument23 pagesDHANRAJDurgesh Patil DspNo ratings yet
- STOK BARANG SAAT INI PT. COMBI PUTRA MANDIRIDocument34 pagesSTOK BARANG SAAT INI PT. COMBI PUTRA MANDIRIAtik Marfu'ahNo ratings yet
- Sub: Refrigeration and Air Conditioning (PE-ME601B) 6 Semester 2021-22Document92 pagesSub: Refrigeration and Air Conditioning (PE-ME601B) 6 Semester 2021-22Amritendu AcharjeeNo ratings yet
- Bearing HousingDocument4 pagesBearing HousingT ThirumuruganNo ratings yet
- Bhopal Gas TragedyDocument14 pagesBhopal Gas Tragedyhriday kumarNo ratings yet
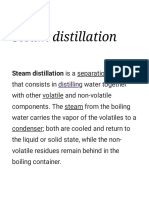
- Steam Distillation - WikipediaDocument16 pagesSteam Distillation - WikipediaAqsa QureshiNo ratings yet