You might also like
- Hematologic DisordersDocument7 pagesHematologic DisordersCernan Oliveros100% (3)
- HY Endocrine UsmleDocument22 pagesHY Endocrine UsmleNakhal JararNo ratings yet
- Grade 12 - Biology Resource BookDocument245 pagesGrade 12 - Biology Resource BookMali100% (6)
- Floor PlansDocument24 pagesFloor PlansSG PropTalkNo ratings yet
- Pediatrics Study GuideDocument22 pagesPediatrics Study GuideElizabeth McKee100% (1)
- Hypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypocalcemia, (Low Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
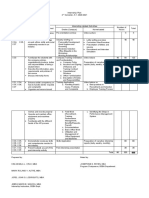
- Internship-Plan BSBA FInalDocument2 pagesInternship-Plan BSBA FInalMark Altre100% (1)
- Sickle Cell Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSickle Cell Anemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Anemia and Pyometra in DogsDocument20 pagesAnemia and Pyometra in DogsVer FajaNo ratings yet
- KMU Blood DisorderDocument43 pagesKMU Blood DisorderSHAFIQNo ratings yet
- Sickle Cell Anemia Nursing Care PlanDocument6 pagesSickle Cell Anemia Nursing Care PlanArisa Vijungco100% (4)
- Type Test Verification SafePlus 12 24 KVDocument8 pagesType Test Verification SafePlus 12 24 KVGary FortuinNo ratings yet
- Aplastic AnemiaDocument16 pagesAplastic Anemiahazelposis100% (1)
- History of Some Special ExplosivesDocument24 pagesHistory of Some Special ExplosivesShazil KhanNo ratings yet
- MS HemaDocument6 pagesMS HemaFrechel Ann Landingin PedrozoNo ratings yet
- Mission and VissionDocument11 pagesMission and VissionPradeep Kumar V PradiNo ratings yet
- Hirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersDocument139 pagesHirschprung's Disease, Celiac Disease, Hydrocephalus, Poisoning, Child Abuse, Anemia, Respiratory DisordersJhoms Poja FeriaNo ratings yet
- Anatomy & Physiology Myelodysplastic Syndrome: PathophysiologyDocument8 pagesAnatomy & Physiology Myelodysplastic Syndrome: PathophysiologyLouise Anne Agnazata GayoNo ratings yet
- Disorders of The BloodDocument35 pagesDisorders of The BloodNoor IbrahimNo ratings yet
- Blood Disorders AnemiaDocument6 pagesBlood Disorders AnemiaFreeNursingNotesNo ratings yet
- AnemiaDocument43 pagesAnemiapradeep pintoNo ratings yet
- Peds HemeImmune OUTLINEDocument10 pagesPeds HemeImmune OUTLINEAshleyNo ratings yet
- Sickle Cell Disease ManagementDocument23 pagesSickle Cell Disease ManagementAndrew SilungweNo ratings yet
- Anemias: Disorders of The Red Blood CellsDocument32 pagesAnemias: Disorders of The Red Blood CellsDthird Mendoza ClaudioNo ratings yet
- Pediatrics RevisedDocument72 pagesPediatrics RevisedShreya SinghNo ratings yet
- Lukes Presentation 1Document28 pagesLukes Presentation 1Lukes GutierrezNo ratings yet
- Hematological DisorderDocument49 pagesHematological DisorderSandeepNo ratings yet
- Sickle Cell Disease: I. Description Including Statistics and IncidencesDocument8 pagesSickle Cell Disease: I. Description Including Statistics and IncidencesMojeca Christy GallaNo ratings yet
- Hematology 101: Hematology/Oncology PG 1 of 11Document12 pagesHematology 101: Hematology/Oncology PG 1 of 11esther100% (1)
- Thalassemia Syndromes: Clinical Features and ComplicationsDocument22 pagesThalassemia Syndromes: Clinical Features and ComplicationsMohamed Al-zichrawyNo ratings yet
- AnemiaDocument6 pagesAnemiaAnsu MaliyakalNo ratings yet
- Hematologic DisorderDocument8 pagesHematologic DisorderRayan AhmedNo ratings yet
- Hematolory Handouts For Iloilo 1 1Document10 pagesHematolory Handouts For Iloilo 1 1Barangay Centro SurNo ratings yet
- Anemia Nursing Care Plan: Presented by Edi Purwanto School of Nursing University of Muhammadiyah MalangDocument26 pagesAnemia Nursing Care Plan: Presented by Edi Purwanto School of Nursing University of Muhammadiyah MalangSevina Eka ChannelNo ratings yet
- Hematolory Handouts For Iloilo 1 1 3Document10 pagesHematolory Handouts For Iloilo 1 1 3Aphrill Pearl PacisNo ratings yet
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 pagesPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNo ratings yet
- Anemia Part IIDocument5 pagesAnemia Part IIChao GeetimoyNo ratings yet
- Hema System 1Document8 pagesHema System 1ErikaNo ratings yet
- He MaDocument25 pagesHe MaBeep TerradoNo ratings yet
- Anemia During PregnancyDocument39 pagesAnemia During PregnancyBhawna JoshiNo ratings yet
- Beta Thalassemia: Types Four FormsDocument8 pagesBeta Thalassemia: Types Four FormsAnsu MaliyakalNo ratings yet
- Hematologic DxsDocument34 pagesHematologic DxsAYTONA, JAMAICA F.No ratings yet
- Management of Patient With AnemiaDocument58 pagesManagement of Patient With AnemiaDoaa HussainNo ratings yet
- Askep Leukimia B.inggrisDocument20 pagesAskep Leukimia B.inggrisAdly BlackNo ratings yet
- Sickle Cell AnemiaDocument21 pagesSickle Cell AnemiaMARA OROPANo ratings yet
- Congenital Blood DisordersDocument32 pagesCongenital Blood DisordersErika CadawanNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic Disorderjulesubayubay5428No ratings yet
- Sisay Berane 083 PancytopeniaDocument23 pagesSisay Berane 083 PancytopeniaRas Siko SafoNo ratings yet
- The Bleeding Child OSCE HaemophiliaDocument3 pagesThe Bleeding Child OSCE HaemophiliaJJ LimNo ratings yet
- Hematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNDocument80 pagesHematology: Jan Bazner-Chandler CPNP, CNS, MSN, RNWarrenPeaceNo ratings yet
- Bone Marrow Failure VoiceoverDocument18 pagesBone Marrow Failure Voiceoverياسر كوثر هانيNo ratings yet
- Anemia Clinical CaseDocument16 pagesAnemia Clinical CaseHoàngBảoLongNo ratings yet
- Saint Luke's College Of: NursingDocument6 pagesSaint Luke's College Of: NursingApril Mae Magos LabradorNo ratings yet
- Approach To HemoglobinopathiesDocument37 pagesApproach To Hemoglobinopathiesabo slo0hNo ratings yet
- Interferences With Diffusion: AnemiaDocument49 pagesInterferences With Diffusion: AnemiaMaryAnn ElizabethNo ratings yet
- Handout 1Document7 pagesHandout 1api-448398971No ratings yet
- Sickle Cell Disease (Diagnosis and Treatment) Copy CopyDocument8 pagesSickle Cell Disease (Diagnosis and Treatment) Copy Copysufian JaganyNo ratings yet
- Sickle - Cell - Guidelines TTTDocument2 pagesSickle - Cell - Guidelines TTTAhmed BadrNo ratings yet
- 101 FullDocument15 pages101 FullhelinNo ratings yet
- UNIT - VI Children With Various DisordersDocument24 pagesUNIT - VI Children With Various Disordersalikalaimchenlar19No ratings yet
- نسخة من HemoglobipathiesDocument63 pagesنسخة من Hemoglobipathiesnour khaleel Mohammad BojaNo ratings yet
- Nephrotic SyndromeDocument34 pagesNephrotic SyndromeAnusikta PandaNo ratings yet
- Ms. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay ProvinceDocument12 pagesMs. Tashmera P. Datukali: Mindanao State University Buug Campus - Ipil Extension Sanito, Ipil, Zamboanga Sibugay Provincesandro2000No ratings yet
- Nephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearDocument28 pagesNephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearMaria YaseenNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- حل اطفال نهائي حمدان حجازيDocument15 pagesحل اطفال نهائي حمدان حجازيIbra NelsonNo ratings yet
- Acute Post Streptococcaالمحاضرة lDocument6 pagesAcute Post Streptococcaالمحاضرة lMGRNo ratings yet
- Chapter - 2 2Document18 pagesChapter - 2 2احمد خالدNo ratings yet
- وظيفة الجهاز الهضميDocument4 pagesوظيفة الجهاز الهضمياحمد خالدNo ratings yet
- EclampsiaDocument9 pagesEclampsiaاحمد خالدNo ratings yet
- Digestive SystemDocument2 pagesDigestive SystemCarmen CajipeNo ratings yet
- Is Implanted in The Lower Uterine Segment So That It Wholly or Partially Covers The Internal CervicalDocument9 pagesIs Implanted in The Lower Uterine Segment So That It Wholly or Partially Covers The Internal Cervicalاحمد خالدNo ratings yet
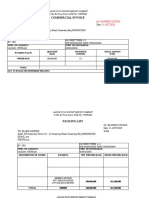
- Invoice, packing list mẫuDocument2 pagesInvoice, packing list mẫuPHI BUI MINHNo ratings yet
- Immulite Homocysteine 2000Document30 pagesImmulite Homocysteine 2000Symbolin MusenkoNo ratings yet
- JECFA Carrageenan MonographDocument5 pagesJECFA Carrageenan MonographSurya SaputraNo ratings yet
- Organisational Behaviour DEC 2022Document10 pagesOrganisational Behaviour DEC 2022Rajni KumariNo ratings yet
- Memorandum - World Safety Day "2023''Document2 pagesMemorandum - World Safety Day "2023''attaullaNo ratings yet
- Benefits of SwimmingDocument3 pagesBenefits of Swimmingaybi pearlNo ratings yet
- Multiple Choice Questions: Topic Covered Are As FollowsDocument3 pagesMultiple Choice Questions: Topic Covered Are As FollowsBikash SahuNo ratings yet
- Shabeer Et Al-2018-Journal of PerinatologyDocument8 pagesShabeer Et Al-2018-Journal of PerinatologyrenataNo ratings yet
- Name of Learner: Section: Subject Teacher: Date:: Practical Research 2Document4 pagesName of Learner: Section: Subject Teacher: Date:: Practical Research 2J-heart Basabas Malpal100% (6)
- The European Board of Anaesthesiology.2Document4 pagesThe European Board of Anaesthesiology.2readririNo ratings yet
- Lab 5 - ReportDocument9 pagesLab 5 - ReportScarlet ErzaNo ratings yet
- Brown Wolf ExerciseDocument8 pagesBrown Wolf ExerciseAarnav kumar0% (1)
- Imaging-Guided Chest Biopsies: Techniques and Clinical ResultsDocument10 pagesImaging-Guided Chest Biopsies: Techniques and Clinical Resultsweni kartika nugrohoNo ratings yet
- IOC CoachingResearchStudiesList PDFDocument87 pagesIOC CoachingResearchStudiesList PDFJeane LucenaNo ratings yet
- Kaul Botanic AllopathyDocument7 pagesKaul Botanic AllopathyabhicwatNo ratings yet
- ProposalDocument3 pagesProposalAbdullahAlmasNo ratings yet
- The Internet Test 9th Grade A2b1 Tests 105573Document5 pagesThe Internet Test 9th Grade A2b1 Tests 105573Daniil CozmicNo ratings yet
- Manual Fritadeira PDFDocument136 pagesManual Fritadeira PDFtherasiaNo ratings yet
- A Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportDocument6 pagesA Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportIJAR JOURNALNo ratings yet
- 94 175 1 SM PDFDocument8 pages94 175 1 SM PDFikaNo ratings yet
- MSDS TSHDocument8 pagesMSDS TSHdwiNo ratings yet
- To: Head of Sea Training Department PT Gemilang Bina Lintas Tirta Ship ManagementDocument1 pageTo: Head of Sea Training Department PT Gemilang Bina Lintas Tirta Ship ManagementtarNo ratings yet
- Operations Manual: Conical Burr Coffee GrinderDocument15 pagesOperations Manual: Conical Burr Coffee Grindercherrera73No ratings yet