You might also like
- 769D Truck & 771D Quarry Truck Electrical System: Machine Harness Connector and Component LocationsDocument2 pages769D Truck & 771D Quarry Truck Electrical System: Machine Harness Connector and Component LocationsGilvan JuniorNo ratings yet
- HIRADC Asphalt RoadDocument1 pageHIRADC Asphalt RoadAshadi Amir100% (1)
- Evaluation of Technopath Controls On The Architect Family of Instruments LittenDocument1 pageEvaluation of Technopath Controls On The Architect Family of Instruments LittenAlyafa LegacyNo ratings yet
- H. Nakano, H. Hashimoto, H. Naraba, M. Mochizuki, Y. Takahashi, T. Sonoo, K. NakamuraDocument1 pageH. Nakano, H. Hashimoto, H. Naraba, M. Mochizuki, Y. Takahashi, T. Sonoo, K. NakamuraViTrieuNo ratings yet
- 8NCEE SanFranciscoDocument11 pages8NCEE SanFranciscojimmy0927802586No ratings yet
- Egger2019 - Nternal Models of Sensorimotor Integration Regulate Cortical DynamicsDocument18 pagesEgger2019 - Nternal Models of Sensorimotor Integration Regulate Cortical DynamicsErick SolisNo ratings yet
- QOL and Cog ImpairementDocument22 pagesQOL and Cog ImpairementDr. Rakesh Kumar TripathiNo ratings yet
- JA2 Post412 ValidityDocument1 pageJA2 Post412 ValidityOscarDavidGordilloGonzalezNo ratings yet
- Conference IADR Africa E-PosterDocument1 pageConference IADR Africa E-PosterAhmed OsamaNo ratings yet
- GROUP 6 - A Study On Attitude and Intention of Indian Youth To Participate in Collaborative ConsumptionDocument9 pagesGROUP 6 - A Study On Attitude and Intention of Indian Youth To Participate in Collaborative ConsumptionBloomy devasiaNo ratings yet
- Regarding The Change of Names Mentioned in The Document, Such As Mitsubishi Electric and Mitsubishi XX, To Renesas Technology CorpDocument10 pagesRegarding The Change of Names Mentioned in The Document, Such As Mitsubishi Electric and Mitsubishi XX, To Renesas Technology CorpTahar BenacherineNo ratings yet
- 2sc4140 Ds enDocument1 page2sc4140 Ds enAdah BumboneNo ratings yet
- 228 Improving Emergency Department Potassium Turnaround TimeDocument1 page228 Improving Emergency Department Potassium Turnaround Timeaboadam aliNo ratings yet
- Silicon NPN Epitaxial Planar Transistor (Complement To Type 2SA1303)Document1 pageSilicon NPN Epitaxial Planar Transistor (Complement To Type 2SA1303)teknikali35No ratings yet
- Evaluation of The HbA1c Kit On Sebia MFP - B. CapolaghiDocument1 pageEvaluation of The HbA1c Kit On Sebia MFP - B. CapolaghiOrlandoNo ratings yet
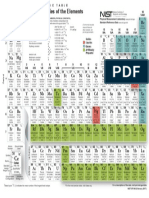
- Atomic Properties of The Elements: GroupDocument1 pageAtomic Properties of The Elements: GroupbarlosNo ratings yet
- Summer Placement Report 2021-23Document8 pagesSummer Placement Report 2021-23SHIVAM BAREJANo ratings yet
- Neuromuscular and Cardiovascular Adaptations In.16Document9 pagesNeuromuscular and Cardiovascular Adaptations In.16Juan Ricardo Sandoval SalcedoNo ratings yet
- Cycle Counting Methods For FatigueDocument7 pagesCycle Counting Methods For FatigueArdiyan Arezel ArdhyNo ratings yet
- D8R II Plano Electrico PDFDocument2 pagesD8R II Plano Electrico PDFDarío Ache EmeNo ratings yet
- D8R Series II Track-Type Tractor Electrical System: Electrical Schematic Symbols and DefinitionsDocument2 pagesD8R Series II Track-Type Tractor Electrical System: Electrical Schematic Symbols and DefinitionsDarío Ache EmeNo ratings yet
- New Sagittal Classification of AIS: Validation by 3D CharacterizationDocument8 pagesNew Sagittal Classification of AIS: Validation by 3D CharacterizationdamonenNo ratings yet
- 23impact of Capital Structure On The Value of The Firm With Reference To Indian PapersDocument9 pages23impact of Capital Structure On The Value of The Firm With Reference To Indian PapersMudit JhunjhunwalaNo ratings yet
- Intelligent Swarm-Based Optimization Technique For Oscillatory Stability Assessment in Power SystemDocument10 pagesIntelligent Swarm-Based Optimization Technique For Oscillatory Stability Assessment in Power SystemIAES IJAINo ratings yet
- 78 Loss of Excitation SIEMENS PaperDocument15 pages78 Loss of Excitation SIEMENS PaperalepreteNo ratings yet
- Silicon NPN Triple Diffused Planar Transistor (High Voltage Switchihg Transistor)Document1 pageSilicon NPN Triple Diffused Planar Transistor (High Voltage Switchihg Transistor)miloud1911No ratings yet
- Hybrid Blade Element and Lifting Line For Propeller or Propfan PerformanceDocument11 pagesHybrid Blade Element and Lifting Line For Propeller or Propfan PerformancewharNo ratings yet
- Pom 10 Years Shiv DasocrDocument115 pagesPom 10 Years Shiv DasocrNavya TandonNo ratings yet
- Evaluation of Total Corneal Power MeasurementsDocument7 pagesEvaluation of Total Corneal Power MeasurementsMariana Luzardo bravoNo ratings yet
- MCEN2000 ThinWallCyclinder 19939889Document12 pagesMCEN2000 ThinWallCyclinder 19939889Mr. Danish SaeedNo ratings yet
- BB M02 - Exercise VSM Student Copy Fixed 2023-3 - NewDocument2 pagesBB M02 - Exercise VSM Student Copy Fixed 2023-3 - NewVíctor Manuel Hernández PNo ratings yet
- 4 Biomechanics of The Vertebral ColumnDocument45 pages4 Biomechanics of The Vertebral ColumnDaniel PereiraNo ratings yet
- Experiment 3 Energy Transformation: Laboratory ReportDocument10 pagesExperiment 3 Energy Transformation: Laboratory ReportDave FortuNo ratings yet
- Measurement System Analysis (MSA) Gauge Repeatability & Reproducibility (GR&R)Document1 pageMeasurement System Analysis (MSA) Gauge Repeatability & Reproducibility (GR&R)Sharif KhanNo ratings yet
- Darlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2389)Document1 pageDarlington: Silicon PNP Epitaxial Planar Transistor (Complement To Type 2SD2389)Gilberto DiazNo ratings yet
- Environmental Protection Agency Pt. 136, App. B: T 6-A E C C / 'Document4 pagesEnvironmental Protection Agency Pt. 136, App. B: T 6-A E C C / 'xacvierNo ratings yet
- Nilai Semester 6 - (Sistem Operasi) - 2018-2019 - (Triyono)Document210 pagesNilai Semester 6 - (Sistem Operasi) - 2018-2019 - (Triyono)Ariyanto Kurniawan PrasetyoNo ratings yet
- Preliminary Copy: Chassis Electrical Circuit Diagram Manual Electrical System Troubleshooting GuideDocument2 pagesPreliminary Copy: Chassis Electrical Circuit Diagram Manual Electrical System Troubleshooting GuideEduardo Torres100% (1)
- Incites Journal Citation Reports-Ieee Transactions On Industrial Electronics-Tier1Document3 pagesIncites Journal Citation Reports-Ieee Transactions On Industrial Electronics-Tier1Thien LeNo ratings yet
- Cecep Mulyana - AK118031 Pert 15 BiostastistikDocument41 pagesCecep Mulyana - AK118031 Pert 15 BiostastistikIseu RahmawatiNo ratings yet
- Rapid Entire Body Assessment (REBA) : Applied Ergonomics May 2000Document6 pagesRapid Entire Body Assessment (REBA) : Applied Ergonomics May 2000Muhammad JawadNo ratings yet
- GRADE 4 2nd Periodical Test ScienceDocument6 pagesGRADE 4 2nd Periodical Test ScienceMARY ROSE FURAGGANANNo ratings yet
- EE669 L2 M2 Review of ConceptsDocument3 pagesEE669 L2 M2 Review of ConceptsNikita MadaviNo ratings yet
- Chassis Electrical Circuit Diagram Manual Electrical System Troubleshooting GuideDocument2 pagesChassis Electrical Circuit Diagram Manual Electrical System Troubleshooting GuideMartinez Andryj100% (3)
- 2SA 1492 REMPLAZO de 2sa1244 Driver Turbo ToyotaDocument1 page2SA 1492 REMPLAZO de 2sa1244 Driver Turbo Toyotadavid silveiraNo ratings yet
- Data 1Document6 pagesData 1AL ROSIDNo ratings yet
- 2SC3263 en 10044835Document2 pages2SC3263 en 10044835Janos NagyNo ratings yet
- Arden 2014Document8 pagesArden 2014MeltemNo ratings yet
- Creating A Reactive Energy Pulse Output Based On The ADE7753Document12 pagesCreating A Reactive Energy Pulse Output Based On The ADE7753api-3744762No ratings yet
- Paper RebaDocument6 pagesPaper RebaALEXANDRA MEDALLIT GAMBOA RODRIGUEZNo ratings yet
- Silicon NPN Triple Diffused Planar Transistor (High Voltage and High Speed Switchihg Transistor)Document1 pageSilicon NPN Triple Diffused Planar Transistor (High Voltage and High Speed Switchihg Transistor)José BenavidesNo ratings yet
- Protection Coordination Study TNB PMUDocument9 pagesProtection Coordination Study TNB PMUMohd Izham Idris100% (1)
- Rapid Entire Body Assessment (REBA) : Applied Ergonomics May 2000Document6 pagesRapid Entire Body Assessment (REBA) : Applied Ergonomics May 2000berliancantikberlianNo ratings yet
- Table of Specifications-3Document5 pagesTable of Specifications-3Aprilyn Alejandrino AcutayanNo ratings yet
- 41 1530347319 - 30-06-2018 PDFDocument9 pages41 1530347319 - 30-06-2018 PDFrahul sharmaNo ratings yet
- GurralaDocument18 pagesGurralaaashnaNo ratings yet
- Wentz Application FinalDocument1 pageWentz Application FinalTaryn BlackstockNo ratings yet
- Taryn S. Blackstock, Alejandra Barrera-Curiel, Jesus Hernandez-Sarabia, Jason M. DefreitasDocument1 pageTaryn S. Blackstock, Alejandra Barrera-Curiel, Jesus Hernandez-Sarabia, Jason M. DefreitasTaryn BlackstockNo ratings yet
- Taryn S. Blackstock, Mitchel A. Magrini, Ryan J Colquhoun, Matthew C. Ferrell, Sydney R. Felming, Nathaniel D.M. Jenkins, Jason M. DefreitasDocument1 pageTaryn S. Blackstock, Mitchel A. Magrini, Ryan J Colquhoun, Matthew C. Ferrell, Sydney R. Felming, Nathaniel D.M. Jenkins, Jason M. DefreitasTaryn BlackstockNo ratings yet
- Research PaperDocument10 pagesResearch PaperTaryn BlackstockNo ratings yet
- Research PosterDocument1 pageResearch PosterTaryn BlackstockNo ratings yet
- 2 Daniel Laskin - Diagnosis and Treatment of MPDSDocument10 pages2 Daniel Laskin - Diagnosis and Treatment of MPDSdocddsNo ratings yet
- Biomedical and Instrumentation Lab FileDocument37 pagesBiomedical and Instrumentation Lab Fileshadan alamNo ratings yet
- The Power of The Mind: The Cortex As A Critical Determinant of Muscle Strength/weaknessDocument8 pagesThe Power of The Mind: The Cortex As A Critical Determinant of Muscle Strength/weaknessHuyentrang VuNo ratings yet
- Facilitatory and Inhibitory Effects of Kinesio TapeDocument4 pagesFacilitatory and Inhibitory Effects of Kinesio TapeFrancisco Javier Luza RamosNo ratings yet
- Comparison of Hamstring Muscle ActivationDocument10 pagesComparison of Hamstring Muscle ActivationDenis SaricNo ratings yet
- Scio and Its Functionality and UsesDocument5 pagesScio and Its Functionality and UsesAndy MilitaruNo ratings yet
- (Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)Document676 pages(Contemporary Neurology Series, 66) Jasper R. Daube - Clinical Neurophysiology (Contemporary Neurology Series, 66) - Oxford University Press, USA (2002)atif.araf.20No ratings yet
- Development of Low-Cost Portable Hand Exoskeleton For Assistive and Rehabilitation PurposesDocument14 pagesDevelopment of Low-Cost Portable Hand Exoskeleton For Assistive and Rehabilitation Purposesgil lerNo ratings yet
- The Basics of ElectromyographyDocument4 pagesThe Basics of ElectromyographyCamila MendezNo ratings yet
- phy-MEDICAL PHYSICSDocument7 pagesphy-MEDICAL PHYSICSLove Bordamonte0% (1)
- Herniated Nucleus PulposusDocument41 pagesHerniated Nucleus PulposusMichael John F. Natividad100% (1)
- A Systematic Review and Meta-Analysis of Common Therapeutic Exercises That Generate Highest Muscle Activity in The Gluteus Medius and Gluteus Minimus SegmentsDocument26 pagesA Systematic Review and Meta-Analysis of Common Therapeutic Exercises That Generate Highest Muscle Activity in The Gluteus Medius and Gluteus Minimus SegmentssamirNo ratings yet
- Gait Asymmetry in Patients With Limb Length DiscrepancyDocument8 pagesGait Asymmetry in Patients With Limb Length DiscrepancyPhooi Yee LauNo ratings yet
- Rowold Hewson 2020 Biofield Frequency Bands Definitions and Group DifferencesDocument10 pagesRowold Hewson 2020 Biofield Frequency Bands Definitions and Group DifferencesPedro LuizNo ratings yet
- Objective Placement Test 1 - Reduced To 19 PagesDocument20 pagesObjective Placement Test 1 - Reduced To 19 PagesMaLeAlvaradoNo ratings yet
- Electromiografo Marca Xltec Modelo Neuromax 1004Document123 pagesElectromiografo Marca Xltec Modelo Neuromax 1004Manuel FloresNo ratings yet
- Electrotherapy 1 Viva QuestionsDocument9 pagesElectrotherapy 1 Viva QuestionsAmaan Shafique100% (2)
- Bio Amp Owner's GuideDocument50 pagesBio Amp Owner's GuideAmador Garcia IIINo ratings yet
- Chronic Low Back Pain Good Clinical Practice GCPDocument341 pagesChronic Low Back Pain Good Clinical Practice GCPTru ManNo ratings yet
- Bab4 - BiopotentialDocument6 pagesBab4 - BiopotentialDefika Fianti0% (1)
- Design The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesDocument8 pagesDesign The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesYASH SANJAY.INGLENo ratings yet
- 2nd Electrotherapy Previous Yrs Question PaperDocument11 pages2nd Electrotherapy Previous Yrs Question PaperSnoove 2021No ratings yet
- Sensors 23 01539 PDFDocument11 pagesSensors 23 01539 PDFB37Vinita KumariNo ratings yet
- Posterior Crossbite and Functional ChangesDocument7 pagesPosterior Crossbite and Functional ChangesFANOR ALFONSO MARTINEZ ARCÓNNo ratings yet
- Brainwave Controlled Wheelchair (BCW)Document5 pagesBrainwave Controlled Wheelchair (BCW)VIVA-TECH IJRINo ratings yet
- Disease Detection Using Bio RoboticsDocument25 pagesDisease Detection Using Bio RoboticsSufail A80% (5)
- Aquatic ResistanceTraining: Acute and Chronic EffectsDocument14 pagesAquatic ResistanceTraining: Acute and Chronic EffectshappystarsNo ratings yet
- J Rehabil Med 2008 Suppl 46: 1-176Document176 pagesJ Rehabil Med 2008 Suppl 46: 1-176vinoth kumar.sNo ratings yet
- Measuring Only Hop Distance During Single Leg Hop Testing Is Insufficient To Detect Deficits in Knee Function After ACL Reconstruction - A Systematic Review and MetaanalysisDocument16 pagesMeasuring Only Hop Distance During Single Leg Hop Testing Is Insufficient To Detect Deficits in Knee Function After ACL Reconstruction - A Systematic Review and MetaanalysisPriscila AraújoNo ratings yet
- Comparison of Muscle Activation Using Various Hand Positions During The Push-Up ExerciseDocument6 pagesComparison of Muscle Activation Using Various Hand Positions During The Push-Up ExerciseJúnior Alvacir CamargoNo ratings yet