You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Service BulletinDocument16 pagesService BulletinFaizani Rahman100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- C-Programming-Class 8Document39 pagesC-Programming-Class 8jack_harishNo ratings yet
- Magnetic Memory Method 1029Document17 pagesMagnetic Memory Method 1029asoooomi_11No ratings yet
- 2 Finishing Works Method Statement For Building ConstructionDocument15 pages2 Finishing Works Method Statement For Building ConstructionElxao XanNo ratings yet
- Karish Newsletter Issue 4 - DECEMBER 2019 FINALDocument11 pagesKarish Newsletter Issue 4 - DECEMBER 2019 FINALJodan AsiborNo ratings yet
- Lab Report 2Document3 pagesLab Report 2Hassan MehmoodNo ratings yet
- Assignment Christianity Chapter 2Document5 pagesAssignment Christianity Chapter 2MohichehraNo ratings yet
- Perusahaan KelurgaDocument19 pagesPerusahaan KelurgaRahmatNo ratings yet
- 03-01-01 - SALSA - TRAIN - IW34 - PM Order For NotificationDocument12 pages03-01-01 - SALSA - TRAIN - IW34 - PM Order For NotificationMiguel MenesesNo ratings yet
- CopyrightsDocument31 pagesCopyrightsxomilaaNo ratings yet
- B1 UNIT 7 Flipped Classroom Video WorksheetDocument1 pageB1 UNIT 7 Flipped Classroom Video WorksheetHamza AlibegovicNo ratings yet
- Calculation Storm PipeDocument10 pagesCalculation Storm PipesenghouNo ratings yet
- "Once Saved Always Saved": Are They Biblical?Document41 pages"Once Saved Always Saved": Are They Biblical?jarrodjohnNo ratings yet
- Actividad Carta Al Director 8 BásicoDocument13 pagesActividad Carta Al Director 8 BásicomariaNo ratings yet
- English: Quarter 2, Wk.3 - Module 1 Give The Appropriate Communicative Styles For Various SituationsDocument11 pagesEnglish: Quarter 2, Wk.3 - Module 1 Give The Appropriate Communicative Styles For Various SituationsRyan Custodio MarcosNo ratings yet
- EN Infonote Frese ALPHA CartridgeDocument2 pagesEN Infonote Frese ALPHA CartridgededeerlandNo ratings yet
- Political Cartoon Lesson PlanDocument9 pagesPolitical Cartoon Lesson PlanNicolas SawickyNo ratings yet
- Nsejs Solved Past Paper 2012 PDFDocument22 pagesNsejs Solved Past Paper 2012 PDFJAYESH SHIVARKARNo ratings yet
- 07 Subject Verb AgreementDocument14 pages07 Subject Verb AgreementMehak SrivastavaNo ratings yet
- Dissertation On Social Media and PoliticsDocument6 pagesDissertation On Social Media and PoliticsBuyCollegePaperOnlineAtlanta100% (1)
- LP in MATHEMATICS 2Document5 pagesLP in MATHEMATICS 2Jessa PabiNo ratings yet
- A Comparison of The Ideal States of PlatDocument16 pagesA Comparison of The Ideal States of PlatSajid Mahsud100% (1)
- VGA Connector - Wikipedia, The Free EncyclopediaDocument3 pagesVGA Connector - Wikipedia, The Free Encyclopedianishatiwari82No ratings yet
- Brunei OverviewDocument29 pagesBrunei OverviewTee MendozaNo ratings yet
- Igate GW040-HDocument1 pageIgate GW040-HThai Son NguyenNo ratings yet
- MebahelDocument2 pagesMebahelPersephoneNo ratings yet
- Matrix-Vector Multiplication: Annika BiermannDocument34 pagesMatrix-Vector Multiplication: Annika BiermannSur3nNo ratings yet
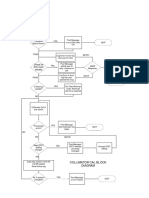
- Check For Dirty Mylar Window: Collimator Cal Block DiagramDocument1 pageCheck For Dirty Mylar Window: Collimator Cal Block DiagramMai Thanh SơnNo ratings yet
- An Empirical Analysis of Money Demand Function in Nepal: Birendra Bahadur BudhaDocument17 pagesAn Empirical Analysis of Money Demand Function in Nepal: Birendra Bahadur BudhaIsmith PokhrelNo ratings yet
- Project 2 Rhetorical Analysis 1Document5 pagesProject 2 Rhetorical Analysis 1api-548504623No ratings yet