You might also like
- Tetralogy of FallotDocument7 pagesTetralogy of FallotWidelmark FarrelNo ratings yet
- Tetralogy of FallotDocument7 pagesTetralogy of FallotAshok Kumar JangirNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Tiki Taka Notes Final PDFDocument104 pagesTiki Taka Notes Final PDFAditiSahak62No ratings yet
- Cyanotic Congenital Heart DiseaseDocument8 pagesCyanotic Congenital Heart DiseaseMohammed Taha Al-nuaimyNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument7 pagesAcyanotic Congenital Heart DiseaseSam Raj100% (1)
- Aruna Ramesh-Emergency...Document6 pagesAruna Ramesh-Emergency...Aishu BNo ratings yet
- Congenital Heart Disease - Cynotic AcynoticDocument34 pagesCongenital Heart Disease - Cynotic Acynoticvruttika parmarNo ratings yet
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseMarisa PetersonNo ratings yet
- Congenital Heart Disease - Part IDocument95 pagesCongenital Heart Disease - Part IMeraol HusseinNo ratings yet
- Cardio Vascular DisordersDocument62 pagesCardio Vascular DisordersUday Kumar100% (1)
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Tetralogy of FallotDocument31 pagesTetralogy of FallotAnditha Namira RS100% (1)
- Cayanotic Heart DiseaseDocument28 pagesCayanotic Heart DiseasesivanathanNo ratings yet
- Congenital Heart Diseases: TopicsDocument19 pagesCongenital Heart Diseases: TopicsMaheen SyedNo ratings yet
- Congenital Heart Disease (2011)Document17 pagesCongenital Heart Disease (2011)drheay100% (1)
- Congenital Heart DefectDocument12 pagesCongenital Heart Defectsangkularosmina837No ratings yet
- Complete Transposition of Great ArteriesDocument85 pagesComplete Transposition of Great ArteriesRahul AgrawalNo ratings yet
- Tof and PdaDocument47 pagesTof and PdaskerstinNo ratings yet
- Tetralogy of FallotDocument28 pagesTetralogy of FallotconcozNo ratings yet
- Cardiovascular DisorderDocument88 pagesCardiovascular DisorderSandeepNo ratings yet
- Ciano Tico IDocument14 pagesCiano Tico ILilik FitrianaNo ratings yet
- K17. Conginetal Heart Disease (Dr. Yanti)Document107 pagesK17. Conginetal Heart Disease (Dr. Yanti)amaliyamataul100% (1)
- Cardiovascular Dysfunction in ChildrenDocument15 pagesCardiovascular Dysfunction in ChildrenJhasseryne Orias SanchezNo ratings yet
- Transposition of Great ArteriesDocument18 pagesTransposition of Great Arteriesparmeshori100% (2)
- Transposition of Great Artery: 1. AbstractDocument7 pagesTransposition of Great Artery: 1. AbstractA. Fajar AprianiNo ratings yet
- Aortopulmonary Window in InfantsDocument3 pagesAortopulmonary Window in Infantsonlyjust4meNo ratings yet
- Tetralogy of Fallot Cyanotic Lesion GuideDocument12 pagesTetralogy of Fallot Cyanotic Lesion Guideputri nadNo ratings yet
- Congenital Heart Disease GuideDocument89 pagesCongenital Heart Disease GuideMathew JosephNo ratings yet
- Cardiovascular System Dr. Eman Badr 2020Document182 pagesCardiovascular System Dr. Eman Badr 2020Amina DinarNo ratings yet
- Current Management of Infants and Children With Single Ventricle AnatomyDocument13 pagesCurrent Management of Infants and Children With Single Ventricle AnatomyjahangirealamNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Stenosis Pulmonal.Document21 pagesStenosis Pulmonal.syelNo ratings yet
- Lapkas Dian and DamboDocument34 pagesLapkas Dian and DamboDian Primadia PutriNo ratings yet
- Cardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNDocument49 pagesCardiovascular Disorders: Prepared By: Wad-Ey, Rosie Glae, RNrosieglaeNo ratings yet
- VSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectDocument53 pagesVSD Guide: Types, Causes and Nursing Care for Ventricular Septal DefectAuni Akif AleesaNo ratings yet
- Child & Adolescent Health Nursing Lecturer Dr. Rayyan's GuideDocument14 pagesChild & Adolescent Health Nursing Lecturer Dr. Rayyan's GuideRayan AhmedNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Acyanoticheartdiseases 180620040047 PDFDocument88 pagesAcyanoticheartdiseases 180620040047 PDFElijahNo ratings yet
- Congenital Heart Disease: Causes, Types, Symptoms and TreatmentDocument69 pagesCongenital Heart Disease: Causes, Types, Symptoms and TreatmentAswathy AswathyNo ratings yet
- Approach To A Child With Congenital Heart DiseaseDocument31 pagesApproach To A Child With Congenital Heart DiseaseMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- Nursing Care Plan For Acyanotic Heart DiseaseDocument55 pagesNursing Care Plan For Acyanotic Heart DiseaseDeepikaxena John79% (14)
- Tricuspid AtresiaDocument44 pagesTricuspid Atresiadoctorsaty7539No ratings yet
- IR 2022 Pediatric Nursing Handouts - Prof. Ma. Teresa VanguardiaDocument15 pagesIR 2022 Pediatric Nursing Handouts - Prof. Ma. Teresa VanguardiaJamie John EsplanadaNo ratings yet
- Atrial Septal Defects: Presented by Dr. Maysa Abdul Haq Directed by Dr. Ali Halabi Jordan Hospital 11-9-2005Document36 pagesAtrial Septal Defects: Presented by Dr. Maysa Abdul Haq Directed by Dr. Ali Halabi Jordan Hospital 11-9-2005Joe JosephNo ratings yet
- (I..) KMU Peads CardicDocument88 pages(I..) KMU Peads CardicMuhammadNo ratings yet
- Ventricular Septal DefectDocument43 pagesVentricular Septal DefectmalekNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- Board Review Pediatrics PDFDocument215 pagesBoard Review Pediatrics PDFJoanne Blanco100% (1)
- Congenital Heart DiseaseDocument22 pagesCongenital Heart DiseasekalpeshjatavNo ratings yet
- 12 - Semiotics of Cardiovascular Disorders. Semiotics of Congenital Hert Diseases in Children.Document30 pages12 - Semiotics of Cardiovascular Disorders. Semiotics of Congenital Hert Diseases in Children.Omowunmi KadriNo ratings yet
- CVS - Session 3 - CHDDocument3 pagesCVS - Session 3 - CHDkotecha.rheaNo ratings yet
- Congenital Heart Disease GuideDocument77 pagesCongenital Heart Disease GuideMalueth Angui100% (1)
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- Congenital Heart DiseasesDocument55 pagesCongenital Heart DiseasesRajaNo ratings yet
- Presented by Dona Mathew MSC (N) Govt - College of Nursing KottayamDocument221 pagesPresented by Dona Mathew MSC (N) Govt - College of Nursing KottayamSumathi GopinathNo ratings yet
- Tetralogy of Fallot, Agarwala 2017Document5 pagesTetralogy of Fallot, Agarwala 2017rinayondaNo ratings yet
- Pediatric Patent Ductus ArteriosusDocument12 pagesPediatric Patent Ductus Arteriosusabirami_murugesuNo ratings yet
- Constitutional Law 2012Document434 pagesConstitutional Law 2012naeemNo ratings yet
- CIMA Business Economics Study Text PDFDocument489 pagesCIMA Business Economics Study Text PDFSimon Chawinga100% (11)
- ACCOUNTS Foundation Paper1Document336 pagesACCOUNTS Foundation Paper1mukni613324100% (1)
- ISSA Corrective ExerciseDocument268 pagesISSA Corrective ExerciseSalman Khan100% (2)
- Ethics and LawDocument321 pagesEthics and LawSalman KhanNo ratings yet
- An Overview of EconomicsDocument17 pagesAn Overview of Economicsveronica_rachnaNo ratings yet
- Orthopedic Congenital and Developmental Conditions in ChildhoodDocument28 pagesOrthopedic Congenital and Developmental Conditions in ChildhoodSalman KhanNo ratings yet
- Spinal Cord Injury ManagementDocument63 pagesSpinal Cord Injury ManagementSalman KhanNo ratings yet
- 185941592XDocument210 pages185941592Xalex_oganesyan100% (7)
- 08 09 2022 Express IslamabadDocument10 pages08 09 2022 Express IslamabadSalman KhanNo ratings yet
- Stroke 15.1Document27 pagesStroke 15.1Salman KhanNo ratings yet
- 1 Neurological RehabilitationDocument20 pages1 Neurological RehabilitationSalman KhanNo ratings yet
- Examination of CoordinationDocument17 pagesExamination of CoordinationSalman KhanNo ratings yet
- 10 StrokeDocument24 pages10 StrokeSalman KhanNo ratings yet
- Neuorlogical Assessment-1Document52 pagesNeuorlogical Assessment-1Salman KhanNo ratings yet
- 4.sensorry ExaminationDocument27 pages4.sensorry ExaminationSalman KhanNo ratings yet
- 1a. Obstetric Emergencies Koros E.KDocument225 pages1a. Obstetric Emergencies Koros E.KSalman KhanNo ratings yet
- 6.motor AssessmentDocument32 pages6.motor AssessmentSalman KhanNo ratings yet
- Neuorlogical AssessmentDocument38 pagesNeuorlogical AssessmentSalman KhanNo ratings yet
- Backache PDFDocument173 pagesBackache PDFteammrau100% (6)
- 4 AsthmaDocument32 pages4 AsthmaSalman KhanNo ratings yet
- 1a. OrthopaedicsDocument19 pages1a. OrthopaedicsSalman KhanNo ratings yet
- Neuorlogical AssessmentDocument41 pagesNeuorlogical AssessmentSalman KhanNo ratings yet
- Burns LectureDocument51 pagesBurns LectureSalman KhanNo ratings yet
- Cerebral Palsy (CP) : Neurology Chapter of IAPDocument42 pagesCerebral Palsy (CP) : Neurology Chapter of IAPWegrimel AriegaraNo ratings yet
- 2.presentation NeuroDocument14 pages2.presentation NeuroSalman KhanNo ratings yet
- The Orthopedic History and Physical Exam GuideDocument28 pagesThe Orthopedic History and Physical Exam GuideAgriya Shresth100% (1)
- Roberta B. Shepherd (Auth.) - Cerebral Palsy in Infancy. Targeted Activity To Optimize Early Growth and Development-Churchill Livingstone (2014) PDFDocument329 pagesRoberta B. Shepherd (Auth.) - Cerebral Palsy in Infancy. Targeted Activity To Optimize Early Growth and Development-Churchill Livingstone (2014) PDFLaura Gallego OrtegaNo ratings yet
- Book 1st Mcqs AllDocument185 pagesBook 1st Mcqs AllSalman KhanNo ratings yet
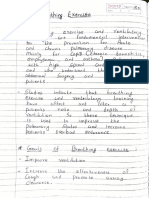
- Breathing Exercises Hand NotesDocument16 pagesBreathing Exercises Hand NotesSalman KhanNo ratings yet
- Trauma Dan Kegawatdaruratan MataDocument92 pagesTrauma Dan Kegawatdaruratan MataM Isyhaduul IslamNo ratings yet
- Exercise 6 Make An Incident Report and Conduct An InvestigationDocument5 pagesExercise 6 Make An Incident Report and Conduct An InvestigationRoxana BaltatescuNo ratings yet
- Risk Factors for Hypertensive Retinopathy: Long Duration and ET-1 LevelDocument6 pagesRisk Factors for Hypertensive Retinopathy: Long Duration and ET-1 Levelfk unswagatiNo ratings yet
- Things To Know About Life Sustaining Treatment4Document3 pagesThings To Know About Life Sustaining Treatment4DurgaPrasadNo ratings yet
- Graph Pharmacology CollectionDocument4 pagesGraph Pharmacology Collectionmanik_ghadlingeNo ratings yet
- Ortho - Perio CasesDocument31 pagesOrtho - Perio CasesChhavi SinghalNo ratings yet
- Lec12 4th ClassDocument8 pagesLec12 4th ClassYaser JasNo ratings yet
- Rehab Centre For DisabledDocument48 pagesRehab Centre For DisabledHanan Mohammed KhalidNo ratings yet
- 個案報告:游離齒突小骨導致後循環復發性中風Document6 pages個案報告:游離齒突小骨導致後循環復發性中風王湘淇No ratings yet
- Asia's leading technical conference for poultry veterinariansDocument4 pagesAsia's leading technical conference for poultry veterinariansnfroyaldeNo ratings yet
- GeneFinder ManualDocument19 pagesGeneFinder ManualbicemanNo ratings yet
- Readers Digest International - March 2017Document130 pagesReaders Digest International - March 2017Alfredo Rafael AcostaNo ratings yet
- Jalak Patel Resume 6-15Document3 pagesJalak Patel Resume 6-15api-288022977No ratings yet
- Test Bank For Essentials of Human Diseases and Conditions 4th Edition FrazierDocument6 pagesTest Bank For Essentials of Human Diseases and Conditions 4th Edition FrazierLinda Abela100% (29)
- Calcium Isotope Ratios in Blood and Urine A New Biomarker For The Diagnosis of OsteoporosisDocument9 pagesCalcium Isotope Ratios in Blood and Urine A New Biomarker For The Diagnosis of OsteoporosisKauã SarinhoNo ratings yet
- Pregnancy Risk Assessment Forms HSEJuly 2015 PDFDocument5 pagesPregnancy Risk Assessment Forms HSEJuly 2015 PDFAndrei Razvan GasparelNo ratings yet
- 4 - Plaque Control MethodsDocument35 pages4 - Plaque Control MethodsDr. Siddana GoudNo ratings yet
- Amaranth Plant of The FutureDocument118 pagesAmaranth Plant of The FutureGabrIela PerezNo ratings yet
- Esubalew AmsaluDocument74 pagesEsubalew AmsaluD100% (2)
- ALCOHOLIMSDocument9 pagesALCOHOLIMSSantiago RamirezNo ratings yet
- Professionalism in NursingDocument10 pagesProfessionalism in NursingFara UmainahNo ratings yet
- Dental Implants - The Best Way To Get Teeth ReplacementDocument3 pagesDental Implants - The Best Way To Get Teeth ReplacementRiya RoyNo ratings yet
- MSDS 741807 Sealant Pipe Loctite 567 56741 250ML PDFDocument4 pagesMSDS 741807 Sealant Pipe Loctite 567 56741 250ML PDFShinta Nugraha MughniNo ratings yet
- Ultrasound-Guided Supraclavicular Brachial Plexus BlockDocument9 pagesUltrasound-Guided Supraclavicular Brachial Plexus Blockfano182No ratings yet
- (Chapman & Hall - CRC Biostatistics) Qingzhao Yu, Bin Li - Statistical Methods For Mediation, Confounding and Moderation Analysis Using R and SAS-CRC Press (2022)Document294 pages(Chapman & Hall - CRC Biostatistics) Qingzhao Yu, Bin Li - Statistical Methods For Mediation, Confounding and Moderation Analysis Using R and SAS-CRC Press (2022)jamalxNo ratings yet
- Chrysonilia Sitophila Growth On Different CultureDocument7 pagesChrysonilia Sitophila Growth On Different CultureDemetriaNo ratings yet
- Book Reviews: Mandibular Suction-Effective Denture and BPS: A Complete GuideDocument1 pageBook Reviews: Mandibular Suction-Effective Denture and BPS: A Complete GuideArjun NarangNo ratings yet
- Abbreviated POMS Questionnaire (Items and Scoring Key) : April 2016Document5 pagesAbbreviated POMS Questionnaire (Items and Scoring Key) : April 2016Karoni100% (1)
- Contraception Chart SexualityDocument8 pagesContraception Chart SexualityRNStudent1No ratings yet
- A Review On: Salmonellosis and Its Economic and Public Health SignificanceDocument13 pagesA Review On: Salmonellosis and Its Economic and Public Health Significanceamanmalako50No ratings yet