You might also like
- The Book of Snakes: A Life-Size Guide to Six Hundred Species from Around the WorldFrom EverandThe Book of Snakes: A Life-Size Guide to Six Hundred Species from Around the WorldRating: 5 out of 5 stars5/5 (1)
- Animal Toxins Zootoxins Snake VenomDocument96 pagesAnimal Toxins Zootoxins Snake VenomSRINIVASAN GnanasabapathyNo ratings yet
- Snake BiteDocument104 pagesSnake Bitenehanirmal0% (1)
- Envenomations: Wonder Abotsi, PHDDocument123 pagesEnvenomations: Wonder Abotsi, PHDKofi Frimpong-Manson100% (1)
- Gigitan Ular: Oleh Alders Allen Kusa NitbaniDocument110 pagesGigitan Ular: Oleh Alders Allen Kusa Nitbanigusty100% (1)
- ParasiteofsnakesinThailand PDFDocument13 pagesParasiteofsnakesinThailand PDFEstefania MoralesNo ratings yet
- Snake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsDocument76 pagesSnake Bite: Abhija Babuji. Crri. Department of Pediatrics. SmimsMeliani FranzNo ratings yet
- A Brief Guide To Snake Envenomations in Malaysia and Antivenom Therapy (Edited)Document18 pagesA Brief Guide To Snake Envenomations in Malaysia and Antivenom Therapy (Edited)ummuawisyNo ratings yet
- Snakebite Symptoms, Causes, and Occupations at RiskDocument95 pagesSnakebite Symptoms, Causes, and Occupations at RisksrinivasNo ratings yet
- An Overview of The Venomous Snakes of TheDocument75 pagesAn Overview of The Venomous Snakes of Thejoks jokaiNo ratings yet
- Discover the diverse world of rove beetlesDocument6 pagesDiscover the diverse world of rove beetlesswahyudi9No ratings yet
- Spiders and Snakes and Things That Slither in The GrassDocument135 pagesSpiders and Snakes and Things That Slither in The GrassJelenaNo ratings yet
- Deadly Snakes: What Are The World's Most Deadly Venomous Snakes?Document5 pagesDeadly Snakes: What Are The World's Most Deadly Venomous Snakes?Rituraj AcharyaNo ratings yet
- Viper SnakeDocument12 pagesViper Snakejayasruthilaya18No ratings yet
- SnakesDocument71 pagesSnakeskf9tqpnkrzNo ratings yet
- Invertebrate in SpaceDocument14 pagesInvertebrate in SpaceRyan HoganNo ratings yet
- Lecture 9.5 Venom (Insect Bite, Snake Bite, Dog Bite)-dr. Akhmad Mahmudi, Sp.B-KBA (2020)Document49 pagesLecture 9.5 Venom (Insect Bite, Snake Bite, Dog Bite)-dr. Akhmad Mahmudi, Sp.B-KBA (2020)stefany huangNo ratings yet
- Snakebite Medan DR DickyDocument37 pagesSnakebite Medan DR Dickypuskesmas paparNo ratings yet
- Snake BiteDocument23 pagesSnake BiteAndika MetrisiawanNo ratings yet
- Update manajemen snakebiteDocument73 pagesUpdate manajemen snakebiteDenny Eka Putri PurwantoNo ratings yet
- Living Fossils: Species That Haven't Changed for Millions of YearsDocument4 pagesLiving Fossils: Species That Haven't Changed for Millions of YearsAYSHAMOHD88No ratings yet
- Phylum Annelida: Segmented Worms With BristlesDocument12 pagesPhylum Annelida: Segmented Worms With BristlesLuthfia PramikaNo ratings yet
- Australian Snake BitesDocument21 pagesAustralian Snake BitesAbubakar BelloNo ratings yet
- Lizard: Jump To Navigationjump To SearchDocument12 pagesLizard: Jump To Navigationjump To SearchLGU-Castilla Raquel J. Dollison, MPDCNo ratings yet
- List of Mammals of The State of PalestineDocument12 pagesList of Mammals of The State of PalestinevalentinoNo ratings yet
- Dragon yDocument147 pagesDragon yBapu MayekarNo ratings yet
- Venomous ArthropodsDocument24 pagesVenomous ArthropodsYuu Ayu'k LifestarNo ratings yet
- Snake: Jump To Navigation Jump To SearchDocument7 pagesSnake: Jump To Navigation Jump To SearchReginald MontanteNo ratings yet
- Cas Common Prohibited ReptilesDocument33 pagesCas Common Prohibited Reptilesdany alarconNo ratings yet
- FleaDocument23 pagesFleaAAREEZ IMRAANNo ratings yet
- Snake Bite Snake Venom Anti-Venom and Herbal AntidDocument8 pagesSnake Bite Snake Venom Anti-Venom and Herbal AntidJohn SnowNo ratings yet
- Full TextDocument59 pagesFull TextMohammed GaberNo ratings yet
- A Scorpion Is An Arthropod With Eight LegsDocument6 pagesA Scorpion Is An Arthropod With Eight LegsyansaagusNo ratings yet
- Scorpion Envenomation: What Is New?: B Rama Chandra ReddyDocument3 pagesScorpion Envenomation: What Is New?: B Rama Chandra ReddyWandarosaliNo ratings yet
- Survey of Mangrove Associated Fauna of Shabi Mangrove Plantation Creek, GwaderDocument23 pagesSurvey of Mangrove Associated Fauna of Shabi Mangrove Plantation Creek, GwaderIrfan AhmadNo ratings yet
- VMP 930 Veterinary Parasitology: Paragonimus KellicottiDocument63 pagesVMP 930 Veterinary Parasitology: Paragonimus KellicottiRenien Khim BahayaNo ratings yet
- Venomous Snake Bites: Iswarya Obilineni Assistant Professor Nirmala College of PharmacyDocument13 pagesVenomous Snake Bites: Iswarya Obilineni Assistant Professor Nirmala College of Pharmacykolipakula venkatNo ratings yet
- Venomous Bites, Stings, and Poisoning: Pablo R. Quedado, MD Unp-College of MedicineDocument9 pagesVenomous Bites, Stings, and Poisoning: Pablo R. Quedado, MD Unp-College of MedicinePrincess Noreen SavellanoNo ratings yet
- Snake Venom ExplainedDocument20 pagesSnake Venom ExplainedManish AmiparaNo ratings yet
- Lecture 1 Introduction InvertDocument36 pagesLecture 1 Introduction Inverthmin1805No ratings yet
- Reptile Bites Guide: Snakebite Risks for FarmersDocument2 pagesReptile Bites Guide: Snakebite Risks for FarmersDesyaNo ratings yet
- 1A Finals Notes (04-04-2022)Document35 pages1A Finals Notes (04-04-2022)Aoun Sial60No ratings yet
- ATLS FatmawatiDocument35 pagesATLS FatmawatiAnindya Anjas PutriaviNo ratings yet
- 016 Fanged + Venomous SnakesDocument563 pages016 Fanged + Venomous SnakesCharlette JauchNo ratings yet
- Bio1AL Diveristy MammalsDocument26 pagesBio1AL Diveristy MammalsThet PhyoeNo ratings yet
- Detection of Parvalbumin A Common Fish Allergen Gene in Food, by Real-Time Polymerase Chain ReactionDocument7 pagesDetection of Parvalbumin A Common Fish Allergen Gene in Food, by Real-Time Polymerase Chain Reactionkhoi moleNo ratings yet
- Poison Apparatus in SnakesDocument13 pagesPoison Apparatus in SnakesGEETA MOHAN100% (2)
- Endoparasites of Pet Reptiles Based On Coprosopic Methods: Original PapersDocument6 pagesEndoparasites of Pet Reptiles Based On Coprosopic Methods: Original PapersCésar Andrés AngelNo ratings yet
- Non-Chordata Animal Kingdom ClassificationDocument71 pagesNon-Chordata Animal Kingdom Classificationasima rath75% (4)
- Sepioloidea Lineolata PDFDocument3 pagesSepioloidea Lineolata PDFenzo abrahamNo ratings yet
- Snake BiteDocument61 pagesSnake Biteniraj_sdNo ratings yet
- EssayDocument4 pagesEssaymigas1996No ratings yet
- The Origin of Complete Metamorphosis: Endopterygota HolometabolaDocument13 pagesThe Origin of Complete Metamorphosis: Endopterygota HolometabolaCarlos Enrique Pijo PerezNo ratings yet
- 4 Poisonous & Venomous AnimalsDocument45 pages4 Poisonous & Venomous AnimalsMarcela GordilloNo ratings yet
- Kelas ChondrichtyesDocument15 pagesKelas ChondrichtyesanitagustinawatiNo ratings yet
- 4 Poisonous & Venomous AnimalsDocument47 pages4 Poisonous & Venomous AnimalsAnyi Yulieth AMPUDIA MURILLONo ratings yet
- Mites: From Wikipedia, The Free EncyclopediaDocument11 pagesMites: From Wikipedia, The Free EncyclopediaTejpal DahiyaNo ratings yet
- Arachnid and Insect VenomDocument56 pagesArachnid and Insect VenomRahmad Budi PrasetyoNo ratings yet
- Entomologi RevisiDocument45 pagesEntomologi RevisiNaomiRimaClaudyaNo ratings yet
- Teams Training GuideDocument12 pagesTeams Training GuideImran HasanNo ratings yet
- LEEA-030.2c2 Certificate of Thorough Examination (Multiple Items) (Overseas) (Dev)Document1 pageLEEA-030.2c2 Certificate of Thorough Examination (Multiple Items) (Overseas) (Dev)GaniyuNo ratings yet
- Year 7 Bugs Lesson 2Document1 pageYear 7 Bugs Lesson 2api-293503824No ratings yet
- Elliott Wave Watching Part 2 Rev 1-2600717Document9 pagesElliott Wave Watching Part 2 Rev 1-2600717GateshNdegwahNo ratings yet
- Ebooks vs Traditional Books: An AnalysisDocument10 pagesEbooks vs Traditional Books: An AnalysisLOVENo ratings yet
- Python operators and data types quizDocument34 pagesPython operators and data types quizATUL SHARMANo ratings yet
- Operational Readiness Guide - 2017Document36 pagesOperational Readiness Guide - 2017albertocm18100% (2)
- MPU 2232 Chapter 5-Marketing PlanDocument27 pagesMPU 2232 Chapter 5-Marketing Plandina azmanNo ratings yet
- Boost productivity and networking with a co-working café in Iligan CityDocument4 pagesBoost productivity and networking with a co-working café in Iligan CityJewel Cabigon0% (1)
- Raoult's law and colligative propertiesDocument27 pagesRaoult's law and colligative propertiesGøbindNo ratings yet
- Quick Reference To Psychotropic Medications: AntidepressantsDocument2 pagesQuick Reference To Psychotropic Medications: AntidepressantsNaiana PaulaNo ratings yet
- Training Report PRASADDocument32 pagesTraining Report PRASADshekharazad_suman85% (13)
- Pro Ducorit UkDocument2 pagesPro Ducorit Uksreeraj1986No ratings yet
- Year 5 Reasoning Test Set 3 Paper A: Q Marks Answer Notes 1a 1b 7 6 4Document2 pagesYear 5 Reasoning Test Set 3 Paper A: Q Marks Answer Notes 1a 1b 7 6 4Amina Zeghar BNo ratings yet
- Product Catalog Encoders en IM0038143Document788 pagesProduct Catalog Encoders en IM0038143Eric GarciaNo ratings yet
- Hercules Segers - Painter EtchterDocument4 pagesHercules Segers - Painter EtchterArtdataNo ratings yet
- Adafruit Color SensorDocument25 pagesAdafruit Color Sensorarijit_ghosh_18No ratings yet
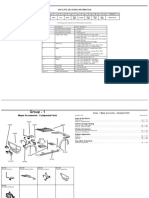
- 2010 - Caliber JEEP BOITE T355Document484 pages2010 - Caliber JEEP BOITE T355thierry.fifieldoutlook.comNo ratings yet
- Cowell - The Wizards of Once PDFDocument315 pagesCowell - The Wizards of Once PDFtatoes n lases100% (1)
- CS Sample Paper 1Document10 pagesCS Sample Paper 1SpreadSheetsNo ratings yet
- PRM Vol1 SystemsDocument1,050 pagesPRM Vol1 SystemsPepe BondiaNo ratings yet
- Asian Paint FMVRDocument20 pagesAsian Paint FMVRdeepaksg787No ratings yet
- Indigo Vision CatalogDocument117 pagesIndigo Vision CatalogWAEL50% (2)
- Timesheet 25Document1 pageTimesheet 25Gwenzieh TugadeNo ratings yet
- TaxonomyDocument56 pagesTaxonomyKrezia Mae SolomonNo ratings yet
- SAP HCM - Default Wage Types - Info Type 0008Document6 pagesSAP HCM - Default Wage Types - Info Type 0008cjherrera2No ratings yet
- Hierarchical Afaan Oromoo News Text ClassificationDocument11 pagesHierarchical Afaan Oromoo News Text ClassificationendaleNo ratings yet
- Gas Mixtures: Seventh Edition in SI UnitsDocument13 pagesGas Mixtures: Seventh Edition in SI Unitshamed farzanehNo ratings yet
- Main Application of Fans and BlowerDocument5 pagesMain Application of Fans and Blowermissy forlajeNo ratings yet
- A An Some Any Jamie Oliver Pancake With Answer KeyDocument8 pagesA An Some Any Jamie Oliver Pancake With Answer Keygcciprian66570% (3)