You might also like
- Matthew J. Friedman (Editor), Paula P. Schnurr (Editor), Terence M. Keane (Editor), Chadi Abdallah (Editor), Garrett B. Aikens (Editor) - Handbook of PTSD - Science and Practice-Guilford Press (2021)Document691 pagesMatthew J. Friedman (Editor), Paula P. Schnurr (Editor), Terence M. Keane (Editor), Chadi Abdallah (Editor), Garrett B. Aikens (Editor) - Handbook of PTSD - Science and Practice-Guilford Press (2021)CESAR DARIO FALCON LIZANO100% (8)
- Exercise and Disease Management Second Edition PDFDocument253 pagesExercise and Disease Management Second Edition PDFGajen Singh100% (1)
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Liver Function TestsDocument16 pagesLiver Function TestsAnjali Devi100% (1)
- Peptic Ulcer Disease: Palangka Raya University Faculty of MedicineDocument70 pagesPeptic Ulcer Disease: Palangka Raya University Faculty of MedicineMITHA100% (1)
- Maxillary Air Sinus Oral SurgeryDocument49 pagesMaxillary Air Sinus Oral SurgeryFourthMolar.com100% (1)
- Samantha Craft's Unofficial Checklist - Females and Autism - Aspergers - The Art of AutismDocument11 pagesSamantha Craft's Unofficial Checklist - Females and Autism - Aspergers - The Art of Autismmiagiles07No ratings yet
- Ampicillin Sodium - Sulbactam Sodium Drug StudyDocument1 pageAmpicillin Sodium - Sulbactam Sodium Drug StudyMelissa Marie Custodio100% (3)
- Volume 15, Number 5 May 2011Document188 pagesVolume 15, Number 5 May 2011Nicolai BabaliciNo ratings yet
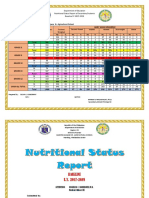
- Nutritional Status Report EndlineDocument3 pagesNutritional Status Report EndlineOliva Cabrales CabornayNo ratings yet
- NEUROLINGUISTICSDocument2 pagesNEUROLINGUISTICSDanny Art'rizhmNo ratings yet
- Symposium of Clinical Neurophysiology 2011Document88 pagesSymposium of Clinical Neurophysiology 2011Snezana Mihajlovic0% (1)
- New Born ClassificationDocument47 pagesNew Born ClassificationEyob MizanNo ratings yet
- Atenolol Drug StudyDocument2 pagesAtenolol Drug StudyFranz.thenurse6888100% (2)
- Ulcerative ColitisDocument9 pagesUlcerative Colitiskint manlangitNo ratings yet
- Dyspepsia Management Guidelines: PrefaceDocument9 pagesDyspepsia Management Guidelines: PrefaceRiefka Ananda ZulfaNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- DYSPHAGIADocument76 pagesDYSPHAGIASaurabh AgarwalNo ratings yet
- Esophageal StrictureDocument6 pagesEsophageal StrictureŽäíñäb ÄljaÑabìNo ratings yet
- Introduction To Gastrointestinal Tract (GIT) : Zheng Shihua The First Clinical Medical College Three Gorge UniversityDocument54 pagesIntroduction To Gastrointestinal Tract (GIT) : Zheng Shihua The First Clinical Medical College Three Gorge UniversityMadhu Sudhan PandeyaNo ratings yet
- Abdome AgudoDocument13 pagesAbdome AgudoJavier VeraNo ratings yet
- Brunner's Gland Adenoma: Case ReportDocument3 pagesBrunner's Gland Adenoma: Case ReportasclepiuspdfsNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- Gastro ActDocument6 pagesGastro Actvincent serquenaNo ratings yet
- Gastrointestinal Surgery 2021Document80 pagesGastrointestinal Surgery 2021Esraa SalemNo ratings yet
- Raj KamalDocument5 pagesRaj KamalBhavani Rao ReddiNo ratings yet
- Perforated Peptic Ulcer Dr. Anbiar Manjas, SP.B-KBDDocument68 pagesPerforated Peptic Ulcer Dr. Anbiar Manjas, SP.B-KBDAndy YusufNo ratings yet
- CabdukadirDocument44 pagesCabdukadirAxmed CumarNo ratings yet
- Intestinal Diseases: Gastrointestinal shengjing Hospital of Medical youwei kou (寇有为)Document80 pagesIntestinal Diseases: Gastrointestinal shengjing Hospital of Medical youwei kou (寇有为)Abhirami AnilNo ratings yet
- Round Table Discussion: Peran Ppi Dalam Manajemen Gastroesophageal Reflux Disease (GERD)Document26 pagesRound Table Discussion: Peran Ppi Dalam Manajemen Gastroesophageal Reflux Disease (GERD)dwi nugroho prastowoNo ratings yet
- Ileus and Bowel ObstructionDocument5 pagesIleus and Bowel ObstructionHayatul AkmaLiaNo ratings yet
- An Overview of Esophageal Disorders (Nour Al-Huda Hamad's Conflicted Copy 2014-07-19)Document16 pagesAn Overview of Esophageal Disorders (Nour Al-Huda Hamad's Conflicted Copy 2014-07-19)Mysheb SSNo ratings yet
- Diagnostic Methods in Dyspepsia The Usefulness of Upper Abdominal Ultrasound and GastrosDocument6 pagesDiagnostic Methods in Dyspepsia The Usefulness of Upper Abdominal Ultrasound and GastrosWingga Chrisna AjiNo ratings yet
- Guidelines On Small Bowel Enteroscopy and Capsule Endoscopy in AdultsDocument12 pagesGuidelines On Small Bowel Enteroscopy and Capsule Endoscopy in Adultssaeed5198No ratings yet
- Open Access Textbook of General Surgery: Large Bowel Obstruction A BoutallDocument6 pagesOpen Access Textbook of General Surgery: Large Bowel Obstruction A BoutallDian FikriNo ratings yet
- Patophsyiology GerdDocument17 pagesPatophsyiology Gerdanon_873909596No ratings yet
- Gastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDocument31 pagesGastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDeep KhemaniNo ratings yet
- Gastro-Oesophageal Reflux Disease: EpidemiologyDocument6 pagesGastro-Oesophageal Reflux Disease: EpidemiologyRehan RiyazNo ratings yet
- Gastro Path yDocument5 pagesGastro Path yAbu RidhuwanNo ratings yet
- Barrett'S Esophagus: Minesh Mehta, PGY-4 University of Louisville Department of GastroenterologyDocument54 pagesBarrett'S Esophagus: Minesh Mehta, PGY-4 University of Louisville Department of Gastroenterologymadhumitha srinivasNo ratings yet
- Oral Exam Gastro 2022Document88 pagesOral Exam Gastro 2022Salih AslaNo ratings yet
- Jurnal TB AbdomenDocument4 pagesJurnal TB AbdomenbelaNo ratings yet
- Research Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaDocument7 pagesResearch Article: Low Prevalence of Clinically Significant Endoscopic Findings in Outpatients With DyspepsiaKurnia pralisaNo ratings yet
- XXXDocument68 pagesXXXUcup SeniorNo ratings yet
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocument24 pagesPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNo ratings yet
- Posterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyDocument7 pagesPosterior Perforation of Gastric Ulcer-A Rare Surgical EmergencyyourinmyheartNo ratings yet
- Diverticular Disease and Intestinal ObstructionDocument31 pagesDiverticular Disease and Intestinal ObstructionPauLa Cheneree Peña ÜNo ratings yet
- Sampling and Reporting of Inflammatory Bowel DiseaseDocument12 pagesSampling and Reporting of Inflammatory Bowel DiseaseDiego Fernando Ortiz TenorioNo ratings yet
- Essay SuryaDocument5 pagesEssay SuryadewasayogaNo ratings yet
- Nissen Fundoplication - StatPearls - NCBI BookshelfDocument9 pagesNissen Fundoplication - StatPearls - NCBI BookshelfAndres Neira QuezadaNo ratings yet
- Merec Briefing No32Document8 pagesMerec Briefing No32Riefka Ananda ZulfaNo ratings yet
- Peptic UlserDocument8 pagesPeptic UlserSubhanshu DadwalNo ratings yet
- Diagnostic Tests: EsophagogastroduodenosDocument6 pagesDiagnostic Tests: EsophagogastroduodenosBereket temesgenNo ratings yet
- Diagnostic Tests: EsophagogastroduodenosDocument6 pagesDiagnostic Tests: EsophagogastroduodenosBereket temesgenNo ratings yet
- Module 1: Gi Topic 1: Esophagus Anatomy and PhysiologyDocument14 pagesModule 1: Gi Topic 1: Esophagus Anatomy and PhysiologyRyan Chistopher UyNo ratings yet
- STOMACCANCEREDITEDDocument12 pagesSTOMACCANCEREDITEDhelloaNo ratings yet
- Peptic Ulcer DiseaseDocument6 pagesPeptic Ulcer DiseaseChino Paolo SamsonNo ratings yet
- JGastr10 GERDDocument8 pagesJGastr10 GERDEnderNo ratings yet
- BY: Amy Rose Abueva, Karyll Chelsea GulfanDocument19 pagesBY: Amy Rose Abueva, Karyll Chelsea GulfanAmy Rose AbuevaNo ratings yet
- Ce 48 291Document6 pagesCe 48 291Siska HarapanNo ratings yet
- Surgical Interventions in Abdominal Tuberculosis: A Clinico-Pathological StudyDocument5 pagesSurgical Interventions in Abdominal Tuberculosis: A Clinico-Pathological StudySatwinder KaurNo ratings yet
- SN 212Document59 pagesSN 212Daroo D.TNo ratings yet
- Complicated Small-Bowel Diverticulosis: A Case Report and Review of The LiteratureDocument3 pagesComplicated Small-Bowel Diverticulosis: A Case Report and Review of The LiteratureYeudiel SuroNo ratings yet
- en Hematochezia in Young Patient Due To CroDocument3 pagesen Hematochezia in Young Patient Due To Croseptian_tjayaNo ratings yet
- Peptic Ulcer Disease - Need PicturesDocument5 pagesPeptic Ulcer Disease - Need PicturesAriana ValenciaNo ratings yet
- Investigations:) - To Diagnose Lesions in The Oesophageal orDocument4 pagesInvestigations:) - To Diagnose Lesions in The Oesophageal orMarwan M.No ratings yet
- Advanced GI Nursing CareDocument13 pagesAdvanced GI Nursing CareBobbi-MarieNo ratings yet
- Inflammatory Bowel DiseaseDocument37 pagesInflammatory Bowel DiseaseDrTushar GoswamiNo ratings yet
- Gastrointestinal Diseases - Part 1Document27 pagesGastrointestinal Diseases - Part 1glenn johnstonNo ratings yet
- Diverticular Disease 2Document5 pagesDiverticular Disease 2karl abiaadNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Primary Sphincter Repair in Anorectal TraumaDocument3 pagesPrimary Sphincter Repair in Anorectal TraumaAhmadNassrNo ratings yet
- Penetrating Anorectal InjuryDocument2 pagesPenetrating Anorectal InjuryAhmadNassrNo ratings yet
- Primary Repair or Fecal Diversion For Colorectal Injuries After Blast A Medical ReviewDocument3 pagesPrimary Repair or Fecal Diversion For Colorectal Injuries After Blast A Medical ReviewAhmadNassrNo ratings yet
- Residents As Teachers of The Pelvic Floor and Perineal AnatomyDocument4 pagesResidents As Teachers of The Pelvic Floor and Perineal AnatomyAhmadNassrNo ratings yet
- Impact of Fecal Incontinence On Quality of LifeDocument7 pagesImpact of Fecal Incontinence On Quality of LifeAhmadNassrNo ratings yet
- Management of Complex Perineal InjuriesDocument6 pagesManagement of Complex Perineal InjuriesAhmadNassrNo ratings yet
- Blunt Pelviperineal InjuriesDocument4 pagesBlunt Pelviperineal InjuriesAhmadNassrNo ratings yet
- Di!cult Colonoscopy: Jerome D. Waye, MDDocument3 pagesDi!cult Colonoscopy: Jerome D. Waye, MDAhmadNassrNo ratings yet
- DR - Ahmed Nassr Teaching Assistant, General Surgery DepDocument33 pagesDR - Ahmed Nassr Teaching Assistant, General Surgery DepAhmadNassrNo ratings yet
- What Is A Difficult ColonosDocument8 pagesWhat Is A Difficult ColonosAhmadNassrNo ratings yet
- The Difficult ColonosDocument8 pagesThe Difficult ColonosAhmadNassrNo ratings yet
- Review of Pelvic Anatomy BMJDocument79 pagesReview of Pelvic Anatomy BMJFilbertaNo ratings yet
- Approach To Incomplete Colonoscopy - New Techniques and Technologies - Gastroenterology & HepatologyDocument15 pagesApproach To Incomplete Colonoscopy - New Techniques and Technologies - Gastroenterology & HepatologyAhmadNassrNo ratings yet
- Pelvic Diaphragm, Urogenital Diaphragm and PerineumDocument30 pagesPelvic Diaphragm, Urogenital Diaphragm and PerineumAhmadNassrNo ratings yet
- 2012 Gemc Res Holliman Abdominal - Pain OerDocument81 pages2012 Gemc Res Holliman Abdominal - Pain OerAhmadNassrNo ratings yet
- Breast Diseases1Document44 pagesBreast Diseases1AhmadNassrNo ratings yet
- Dr. Kanupriya ChaturvediDocument67 pagesDr. Kanupriya ChaturvediAhmadNassrNo ratings yet
- Minerals 1Document92 pagesMinerals 1AhmadNassrNo ratings yet
- IV Solutions Reference Chart Uses Effects PDFDocument1 pageIV Solutions Reference Chart Uses Effects PDFAhmadNassrNo ratings yet
- MalingeringDocument4 pagesMalingeringAnnamalai OdayappanNo ratings yet
- Nutrients: Obesity and Dyslipidemia in South AsiansDocument26 pagesNutrients: Obesity and Dyslipidemia in South AsiansFitriNo ratings yet
- 4.cough and Difficulty of BreathingDocument52 pages4.cough and Difficulty of BreathingLunaLureNo ratings yet
- Review of LitreatureDocument10 pagesReview of Litreaturekuttivasanth50% (2)
- Covid Report: Mr. Rakesh SharmaDocument1 pageCovid Report: Mr. Rakesh Sharmavishal sharmaNo ratings yet
- Service Annotated BibDocument3 pagesService Annotated Bibapi-302015493No ratings yet
- MycosesDocument2 pagesMycosesMadabout MusicNo ratings yet
- Fungal Infections Are More Common Caused byDocument28 pagesFungal Infections Are More Common Caused byPrashun Shekhar SrivastavaNo ratings yet
- Extent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFDocument26 pagesExtent of Compliance To Immunization Reasons For Non Continuity and Its Consequences PDFAPRIL LYNNo ratings yet
- GastrointestinaldrugsDocument30 pagesGastrointestinaldrugsmayaNo ratings yet
- Soal Trik Cepat Utbk B Inggris Part 1Document10 pagesSoal Trik Cepat Utbk B Inggris Part 1Sofia AfrianiNo ratings yet
- Lessons From Social Psychology On Discrediting Psychiatric StigmaDocument12 pagesLessons From Social Psychology On Discrediting Psychiatric Stigmashah khalidNo ratings yet
- Cerebral PalsyDocument96 pagesCerebral PalsyRahini PaniNo ratings yet
- A Patient With Dry Mouth PDFDocument6 pagesA Patient With Dry Mouth PDFWahdatNo ratings yet
- Psychiatric Interview Professor Safeya Effat: I History Taking 1. Personal DataDocument4 pagesPsychiatric Interview Professor Safeya Effat: I History Taking 1. Personal DataAcha Angel BebexzNo ratings yet
- Ερωτήσεις διάφορεςDocument108 pagesΕρωτήσεις διάφορεςyiafkaNo ratings yet
- C 13Document11 pagesC 13Jo100% (1)
- EscitalopramDocument1 pageEscitalopramRicky Ramos Jr.No ratings yet
- Advances in Coeliac Disease: ReviewDocument9 pagesAdvances in Coeliac Disease: ReviewCamilo ReyesNo ratings yet