You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Assessment of Chest and LungsDocument23 pagesAssessment of Chest and LungsBaniwas Marie Agnes100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Global Polio Eradication: History, Achievements & ChallengesDocument59 pagesGlobal Polio Eradication: History, Achievements & ChallengesfahimalikNo ratings yet
- Medical Astrology Part 1Document21 pagesMedical Astrology Part 1Himanshu SharmaNo ratings yet
- Autism Spectrum DisorderDocument33 pagesAutism Spectrum Disorderfcb rmaNo ratings yet
- Aortic AneurysmDocument8 pagesAortic AneurysmShen ParilNo ratings yet
- Maxillary Air Sinus Oral SurgeryDocument49 pagesMaxillary Air Sinus Oral SurgeryFourthMolar.com100% (1)
- Anatomical Zodiacal Degrees PDFDocument6 pagesAnatomical Zodiacal Degrees PDFMaria Marissa100% (2)
- Penyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUDocument56 pagesPenyakit Ginjal Kronik Dan Indikasi Dialisis DR Ratih Tri KD MAJUFitriana WijayatiNo ratings yet
- Trigger Point InjectionDocument10 pagesTrigger Point Injectionv_vijayakanth7656No ratings yet
- A Case Presentation On PneumoniaDocument20 pagesA Case Presentation On PneumoniaCamille Honeyleith Lanuza Fernando80% (5)
- Nipa Virus InfectionsDocument83 pagesNipa Virus Infectionsanon_547200245No ratings yet
- Syphilis Presentation 1Document10 pagesSyphilis Presentation 1fahimalikNo ratings yet
- Poliomyelitis: By: Reema I. DabbasDocument35 pagesPoliomyelitis: By: Reema I. DabbasReema DabbasNo ratings yet
- Sis 06Document9 pagesSis 06fahimalikNo ratings yet
- 4f36powerpoint File Present by DR Wilsom Lam QEH (Updated 030603pm)Document52 pages4f36powerpoint File Present by DR Wilsom Lam QEH (Updated 030603pm)fahimalikNo ratings yet
- Pakistan Floods InformationDocument17 pagesPakistan Floods InformationfahimalikNo ratings yet
- Pakistan Floods July-August 2010: Just-in-Time LectureDocument40 pagesPakistan Floods July-August 2010: Just-in-Time LecturefahimalikNo ratings yet
- DENGUE Fever CartoonDocument15 pagesDENGUE Fever CartoonfahimalikNo ratings yet
- Collaborative Course On Infectious Diseases: Lecture # 4 Dengue FeverDocument54 pagesCollaborative Course On Infectious Diseases: Lecture # 4 Dengue FeverfahimalikNo ratings yet
- HINARI Short Course English 03 2009Document128 pagesHINARI Short Course English 03 2009fahimalikNo ratings yet
- Dengue:: How Are We Doing?Document63 pagesDengue:: How Are We Doing?fahimalikNo ratings yet
- Infectious Diseases: A Global ViewDocument77 pagesInfectious Diseases: A Global View0788950966No ratings yet
- Dengue PosterDocument6 pagesDengue PosterfahimalikNo ratings yet
- Dengue Virus: No One Is Safe: Caitlin Reed Smith College April 29, 2005Document50 pagesDengue Virus: No One Is Safe: Caitlin Reed Smith College April 29, 2005fahimalikNo ratings yet
- Dengue Fever 2Document21 pagesDengue Fever 2dr9348345000No ratings yet
- FloodDocument17 pagesFloodfahimalikNo ratings yet
- Vector Borne Diseases in PakistanDocument21 pagesVector Borne Diseases in PakistanfahimalikNo ratings yet
- Diabetes - The Condition: - What Is It? - How Is It Caused? - Who Gets It? - Risk FactorsDocument20 pagesDiabetes - The Condition: - What Is It? - How Is It Caused? - Who Gets It? - Risk FactorsfahimalikNo ratings yet
- Dengue FeverDocument39 pagesDengue FeverMuhammad Alauddin Sarwar100% (15)
- C081thyroid Present (Shuvro)Document26 pagesC081thyroid Present (Shuvro)fahimalikNo ratings yet
- National AIDS Control Program: Dr. Kanupriya ChaturvediDocument42 pagesNational AIDS Control Program: Dr. Kanupriya ChaturvedifahimalikNo ratings yet
- Stress Management: Allan Sanders, MN, ARNP Asanders@wsu - EduDocument33 pagesStress Management: Allan Sanders, MN, ARNP Asanders@wsu - EdufahimalikNo ratings yet
- 4f36powerpoint File Present by DR Wilsom Lam QEH (Updated 030603pm)Document52 pages4f36powerpoint File Present by DR Wilsom Lam QEH (Updated 030603pm)fahimalikNo ratings yet
- Pakistan Floods July-August 2010: Just-in-Time LectureDocument40 pagesPakistan Floods July-August 2010: Just-in-Time LecturefahimalikNo ratings yet
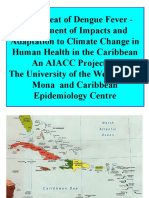
- Presentation Slides: Health and Climate ChangeDocument24 pagesPresentation Slides: Health and Climate ChangeSouth East Asia Regional DelegationNo ratings yet
- Increased Intracranial PressureDocument1 pageIncreased Intracranial PressureFredie O HadjimudinNo ratings yet
- Magic Wave July 2011 PDF 69Document19 pagesMagic Wave July 2011 PDF 69Budi TurmokoNo ratings yet
- FORMAT Discharge PlanDocument5 pagesFORMAT Discharge PlanButchay LumbabNo ratings yet
- Salicylate Intoxication in An Infant: A Case Report: Key PointsDocument5 pagesSalicylate Intoxication in An Infant: A Case Report: Key PointsAna MariaNo ratings yet
- Grade 5 Term 1 SchemeDocument203 pagesGrade 5 Term 1 SchemeConistance GatsiNo ratings yet
- Decreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)Document88 pagesDecreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)leenaNo ratings yet
- 741 PUB Working Paper 35 PDFDocument34 pages741 PUB Working Paper 35 PDFBushra AsifNo ratings yet
- Ka-En MimsDocument7 pagesKa-En MimsMFWPNo ratings yet
- EscitalopramDocument1 pageEscitalopramRicky Ramos Jr.No ratings yet
- Anesthesia For GeriatricDocument21 pagesAnesthesia For GeriatricintanNo ratings yet
- Camp Highland - Adult Medical-Liability FormDocument1 pageCamp Highland - Adult Medical-Liability FormMark AdamsNo ratings yet
- General Surgery Topic ListDocument2 pagesGeneral Surgery Topic Listalijax522No ratings yet
- A. The Sum of All Chemical Reactions in The Organisms, That Produce Energy or Synthesize Organic MatterDocument5 pagesA. The Sum of All Chemical Reactions in The Organisms, That Produce Energy or Synthesize Organic MatterShane Aileen AngelesNo ratings yet
- Safety Precautions For Attending Theocratic SchoolsDocument2 pagesSafety Precautions For Attending Theocratic SchoolsRitaNo ratings yet
- PE 12 Chapter 3Document16 pagesPE 12 Chapter 3Ayisha AlamNo ratings yet
- Chronic Obstructive Pulmonary Disease: Saja QuzmarDocument28 pagesChronic Obstructive Pulmonary Disease: Saja Quzmarkolakav107No ratings yet
- English Diarrhea FixDocument20 pagesEnglish Diarrhea FixLa fazaNo ratings yet
- 702-Article Text-4600-1-10-20181128Document162 pages702-Article Text-4600-1-10-20181128Sampath RavulaNo ratings yet
- Review of LitreatureDocument10 pagesReview of Litreaturekuttivasanth50% (2)