You might also like
- FINAL Food Addiction Tool Kit 10-14-15Document59 pagesFINAL Food Addiction Tool Kit 10-14-15Torc Steele100% (1)
- Culture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewDocument49 pagesCulture and Nonverbal Expressions of Empathy in Clinical Settings - A Systematic ReviewAlberto JaramilloNo ratings yet
- Lesson 1Document8 pagesLesson 1Random RandomNo ratings yet
- FINAL PalliativeCareModule PDFDocument51 pagesFINAL PalliativeCareModule PDFruhyanaNo ratings yet
- Amosup HandbookDocument20 pagesAmosup HandbookHERMAN DAGIO100% (1)
- About The Measure Domain MeasureDocument3 pagesAbout The Measure Domain MeasureMaríaA.SerranoNo ratings yet
- UN Doctors Directory 2015Document18 pagesUN Doctors Directory 2015Kush GuptaNo ratings yet
- Critical Care NursingDocument12 pagesCritical Care NursingMoni Mbumba MelekeNo ratings yet
- Bowel Obstruction PathophysiologyDocument4 pagesBowel Obstruction PathophysiologyAya BolinasNo ratings yet
- Integrative Support and Interprofessional Collaboration in Palliative Care ServicesDocument56 pagesIntegrative Support and Interprofessional Collaboration in Palliative Care Servicesrose fania100% (1)
- The IAHPC Manual of Palliative Care 3eDocument131 pagesThe IAHPC Manual of Palliative Care 3eShadowboroNo ratings yet
- Palliative 1 6Document9 pagesPalliative 1 6Daryl Santiago Delos ReyesNo ratings yet
- Danielle Doberman Geriatric Palliative CareDocument46 pagesDanielle Doberman Geriatric Palliative CareArsya WinaNo ratings yet
- Palliative Care NotesDocument29 pagesPalliative Care NotesCnette S. Lumbo100% (1)
- Cure Palliative 1Document64 pagesCure Palliative 1Mr. LNo ratings yet
- NHS Lanarkshire Palliative Care GuidelinesDocument82 pagesNHS Lanarkshire Palliative Care GuidelinesAndi WiraNo ratings yet
- Research in Palliative Care PresentationDocument20 pagesResearch in Palliative Care PresentationNICKY SAMBONo ratings yet
- Atlas Palliative Care in Europe 2013 PDFDocument410 pagesAtlas Palliative Care in Europe 2013 PDFeduard rusuNo ratings yet
- WHO Generic Palliative Care (Dr. Rudi)Document26 pagesWHO Generic Palliative Care (Dr. Rudi)Inna RosdyasariNo ratings yet
- Pocket Guide To 2015 Beers Criteria PDFDocument7 pagesPocket Guide To 2015 Beers Criteria PDFYuliEdySeringnyungsepNo ratings yet
- Reflection About Palliative Care and End of Life CareDocument5 pagesReflection About Palliative Care and End of Life CareVILLEJO JHOVIALENNo ratings yet
- HOSPICE CARE: A TEAM APPROACH TO COMPASSIONATE END-OF-LIFE CAREDocument7 pagesHOSPICE CARE: A TEAM APPROACH TO COMPASSIONATE END-OF-LIFE CAREJason SteelNo ratings yet
- Caring at The End of Life - Approaching Death - NCBI Bookshelf PDFDocument18 pagesCaring at The End of Life - Approaching Death - NCBI Bookshelf PDFBelaislam Belaulama100% (1)
- Nursing Prioritization of The Patient Ne PDFDocument13 pagesNursing Prioritization of The Patient Ne PDFBambim TexonNo ratings yet
- End of Life CareDocument11 pagesEnd of Life CareBelindaNo ratings yet
- OWL at Purdue University Printable Handouts Using American Psychological Association (APA) FormatDocument28 pagesOWL at Purdue University Printable Handouts Using American Psychological Association (APA) Formatrryan100% (3)
- Assessing Patients and Managing Acute SituationDocument27 pagesAssessing Patients and Managing Acute SituationCHONANo ratings yet
- Bedside Med HX Maker PDFDocument2 pagesBedside Med HX Maker PDFjustinryanNo ratings yet
- Manage Cellulitis at HomeDocument2 pagesManage Cellulitis at HomeAnonymous 4txA8N8etNo ratings yet
- Kerala's Palliative Care Policy ObjectivesDocument33 pagesKerala's Palliative Care Policy Objectivesjajaja hshsjsNo ratings yet
- Trainin On Compassionate, Respectful and Caring Health ProfessionalsDocument21 pagesTrainin On Compassionate, Respectful and Caring Health ProfessionalsnibretzwNo ratings yet
- A Syllabus For Fellowship Education in Palliative MedicineDocument12 pagesA Syllabus For Fellowship Education in Palliative Medicinebaixinha_No ratings yet
- End-Stage Liver DiseaseDocument26 pagesEnd-Stage Liver DiseaseZulvina FaozanudinNo ratings yet
- 1rika Konsep PaliatifDocument47 pages1rika Konsep PaliatifRahmi Ferdila Comate SoniqNo ratings yet
- Critical Care Nursing Responsibilities and SkillsDocument47 pagesCritical Care Nursing Responsibilities and SkillsAamirNo ratings yet
- Palliative CourseDocument98 pagesPalliative Coursejjpuliken100% (1)
- Palliative CareDocument23 pagesPalliative CareCharles Frank100% (1)
- FinalintegrativereviewDocument17 pagesFinalintegrativereviewapi-346349076No ratings yet
- Palliative and Terminal CareDocument78 pagesPalliative and Terminal CareMarivic DianoNo ratings yet
- CARDIOPULMONARY ASSESSMENT AND REHABILITATIONDocument51 pagesCARDIOPULMONARY ASSESSMENT AND REHABILITATIONPreciousShaizNo ratings yet
- Improving The Quality of Care in An Acute Care Facility Through RDocument88 pagesImproving The Quality of Care in An Acute Care Facility Through RNor-aine Salazar AccoyNo ratings yet
- Palliative Care and Islamic Ethics: Exploring Key Issues and Best PracticeDocument54 pagesPalliative Care and Islamic Ethics: Exploring Key Issues and Best PracticeMoosa MohamedNo ratings yet
- ICU MED1 Survival Kits 2009 (Final)Document88 pagesICU MED1 Survival Kits 2009 (Final)Kevin WongNo ratings yet
- Geriatric Giants: Mobility, Incontinence and FallsDocument83 pagesGeriatric Giants: Mobility, Incontinence and FallsSarah Shadiqa100% (1)
- Counselling, Breaking Bad NewsDocument26 pagesCounselling, Breaking Bad NewsArief NorddinNo ratings yet
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansDocument11 pagesCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessNo ratings yet
- Choosing Wisely Master ListDocument92 pagesChoosing Wisely Master ListrobertojosesanNo ratings yet
- WHO Definition of Palliative CareDocument6 pagesWHO Definition of Palliative CareDefri RahmanNo ratings yet
- Providing Culturally Appropriate Care: A Literature ReviewDocument9 pagesProviding Culturally Appropriate Care: A Literature ReviewLynette Pearce100% (1)
- Rns Can Work in A Variety of Healthcare Settings, IncludingDocument6 pagesRns Can Work in A Variety of Healthcare Settings, IncludingpriyagerardNo ratings yet
- Islam and Palliative CareDocument16 pagesIslam and Palliative CareShirakawa AlmiraNo ratings yet
- Original EssayDocument3 pagesOriginal EssayAj AquinoNo ratings yet
- Top 10 Factors For End-Of-Life CareDocument14 pagesTop 10 Factors For End-Of-Life CareJoyce DreuNo ratings yet
- The Nursing Health HistoryDocument25 pagesThe Nursing Health HistoryJonah R. MeranoNo ratings yet
- Role of nurses in global palliative careDocument6 pagesRole of nurses in global palliative care_astyNo ratings yet
- Govt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeDocument17 pagesGovt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeMamta YadavNo ratings yet
- Mask19Document8 pagesMask19steven saputraNo ratings yet
- Alzheimer's Facts & Figures ReportDocument80 pagesAlzheimer's Facts & Figures ReportTime Warner Cable NewsNo ratings yet
- Evidence-Based Practice: The 5 Steps Nurses Need to Provide Quality CareDocument43 pagesEvidence-Based Practice: The 5 Steps Nurses Need to Provide Quality CareApRil Anne Balanon100% (1)
- Palliative Medicine and Supportive CareDocument12 pagesPalliative Medicine and Supportive CareKaren CárcamoNo ratings yet
- Critical Care Nursing EssentialsDocument42 pagesCritical Care Nursing Essentialsikram ullah khanNo ratings yet
- Palliative CareDocument36 pagesPalliative CareAzka Revan0% (1)
- Volunteering in Palliative Care at MTMHDocument17 pagesVolunteering in Palliative Care at MTMHpradeep100% (1)
- DR Pradeep Kulkarni, M.D. (Anaeshesiology) LMRC, PuneDocument31 pagesDR Pradeep Kulkarni, M.D. (Anaeshesiology) LMRC, PunepradeepNo ratings yet
- Ethical Issues - Caring For CaregiverDocument15 pagesEthical Issues - Caring For CaregiverpradeepNo ratings yet
- Gericon Presentation 14-7-2018Document88 pagesGericon Presentation 14-7-2018pradeepNo ratings yet
- My Care My RightDocument42 pagesMy Care My RightpradeepNo ratings yet
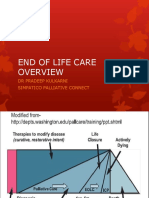
- End of Life Care PresentationDocument50 pagesEnd of Life Care PresentationpradeepNo ratings yet
- Advance Directives Malbar Hill Club 21-4-2018Document51 pagesAdvance Directives Malbar Hill Club 21-4-2018pradeepNo ratings yet
- Doctor Patient RelationshipDocument24 pagesDoctor Patient RelationshippradeepNo ratings yet
- End of Life Care CounsellingDocument24 pagesEnd of Life Care CounsellingpradeepNo ratings yet
- Advance CommunicationDocument22 pagesAdvance CommunicationpradeepNo ratings yet
- Iapc November 2016 Pain PathophysiologyDocument45 pagesIapc November 2016 Pain PathophysiologypradeepNo ratings yet
- Brief Overview of Palliative CareDocument42 pagesBrief Overview of Palliative CarepradeepNo ratings yet
- Case Pres TamparanDocument22 pagesCase Pres TamparanAlano S. LimgasNo ratings yet
- Acute Prescribing - Challenges and Solutions - Ajit KulkarniDocument51 pagesAcute Prescribing - Challenges and Solutions - Ajit KulkarniAgha QaimiNo ratings yet
- HDFC Life Group Credit Protect Plus Insurance Plan20161128 093336 PDFDocument8 pagesHDFC Life Group Credit Protect Plus Insurance Plan20161128 093336 PDFSara LopezNo ratings yet
- Approach To Hemolytic AnemiasDocument41 pagesApproach To Hemolytic AnemiasAmit KinareNo ratings yet
- Skilled Birth Attendant Neonatal Resuscitation Training ProgramDocument48 pagesSkilled Birth Attendant Neonatal Resuscitation Training ProgramPradeep VermaNo ratings yet
- Hypertension in PregnancyDocument8 pagesHypertension in PregnancyCarolina NauNo ratings yet
- First Aid Chapter 1 (Part 1)Document33 pagesFirst Aid Chapter 1 (Part 1)Annie KhorNo ratings yet
- Fact Sheet on Emerging and Re-Emerging Infectious DiseasesDocument7 pagesFact Sheet on Emerging and Re-Emerging Infectious DiseasesAmanda PratiwiNo ratings yet
- Test Bank For Pharmacology For Nurses A Pathophysiologic Approach 5th EditionDocument36 pagesTest Bank For Pharmacology For Nurses A Pathophysiologic Approach 5th Editiontipsterchegoe.t8rlzv100% (41)
- OB Quiz 1: Nishath Sarwath's 10-question OB nursing examDocument5 pagesOB Quiz 1: Nishath Sarwath's 10-question OB nursing examNishath SarwathNo ratings yet
- CPG Labor and Delivery 2015Document78 pagesCPG Labor and Delivery 2015TintalleNo ratings yet
- Manage Expired and Slow Moving InventoryDocument7 pagesManage Expired and Slow Moving InventoryIdan RidwanNo ratings yet
- Emergency Eye Care WorkshopDocument21 pagesEmergency Eye Care WorkshopAriani Ratri Dewi100% (1)
- Cuijpers (2008) Psychological Treatment of Depression A Meta-Analytic Database ofDocument6 pagesCuijpers (2008) Psychological Treatment of Depression A Meta-Analytic Database ofThamara Tapia-MunozNo ratings yet
- LEC 1 Microbiology Intro and Hx. Lec 1Document62 pagesLEC 1 Microbiology Intro and Hx. Lec 1nicewanNo ratings yet
- 01 - Introduction To DentistryDocument18 pages01 - Introduction To Dentistrymichal ben meronNo ratings yet
- Deep Fungal InfectionsDocument33 pagesDeep Fungal Infectionstummalapalli venkateswara raoNo ratings yet
- Recalls 10 - Np2Document6 pagesRecalls 10 - Np2Nova Clea BoquilonNo ratings yet
- Questions from the Ministry of Health for Residency and Fellowship Programs (2013-2018Document68 pagesQuestions from the Ministry of Health for Residency and Fellowship Programs (2013-2018Ahmad HamdanNo ratings yet
- IPAC Checklist for Clinical Office PracticeDocument24 pagesIPAC Checklist for Clinical Office PracticeBABBY ZBOURGNo ratings yet
- CP For Eye NurseDocument3 pagesCP For Eye NursemelanNo ratings yet
- Diagnosing Pompe Disease (Also Known As AcidDocument4 pagesDiagnosing Pompe Disease (Also Known As Aciddonnal47No ratings yet
- Drinking Water and Losing WeightDocument3 pagesDrinking Water and Losing WeightMathana SuriaNo ratings yet
- EMR Implementation Readiness Assessment and Patient Satisfaction ReportDocument20 pagesEMR Implementation Readiness Assessment and Patient Satisfaction ReportAbidi HichemNo ratings yet