You might also like
- R1150RT IABS Electric Diagram V1.0Document3 pagesR1150RT IABS Electric Diagram V1.0Zeljko Tanasic50% (2)
- CentrifugalCompressor5 (1) SelectionDocument5 pagesCentrifugalCompressor5 (1) SelectionbsssnivasNo ratings yet
- Electromagnetic TheoryDocument35 pagesElectromagnetic Theorytareq omarNo ratings yet
- A PPT On Accelerated Stability StudiesDocument16 pagesA PPT On Accelerated Stability StudiesShrikanth Varma Bandi100% (2)
- Suara Jantung 2Document13 pagesSuara Jantung 2Tesis Maruli Tua SianiparNo ratings yet
- Heart Murmurs - Yani YuliaDocument40 pagesHeart Murmurs - Yani YuliayuliaNo ratings yet
- Suara JantungDocument12 pagesSuara JantungTesis Maruli Tua SianiparNo ratings yet
- Systolic Murmurs: DR Muhammed Aslam Junior Resident Pulmonary Medicine ACME PariyaramDocument39 pagesSystolic Murmurs: DR Muhammed Aslam Junior Resident Pulmonary Medicine ACME PariyaramPriyanshiSharmaNo ratings yet
- Cardiac MurmursDocument20 pagesCardiac MurmursFitri Nurullah100% (1)
- Physical Examination of CVDocument40 pagesPhysical Examination of CVNur Hikmah KusumaNo ratings yet
- Approach To Heart MurmursDocument57 pagesApproach To Heart MurmursRadley Jed PelagioNo ratings yet
- Kardio ExamDocument34 pagesKardio ExamsriworoNo ratings yet
- Cardiovascular Examination: Andi Wahjono Adi, MD, FihaDocument34 pagesCardiovascular Examination: Andi Wahjono Adi, MD, FihaAmira FRNo ratings yet
- Cardiology Part PX FisikDocument36 pagesCardiology Part PX FisikNC DieselNo ratings yet
- Tutorial 8 Cardiac ExamDocument14 pagesTutorial 8 Cardiac Examcindy100% (1)
- Cardiac Cycle: Heart Murmurs: Mary Beth Fontana MDDocument43 pagesCardiac Cycle: Heart Murmurs: Mary Beth Fontana MDlessank12No ratings yet
- Heart SoundDocument29 pagesHeart Sounddianpratiwirahim100% (1)
- Heart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreDocument46 pagesHeart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreChenii RoyNo ratings yet
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNo ratings yet
- Physical Examination of The Cardiovascular SystemDocument40 pagesPhysical Examination of The Cardiovascular SystemMyra Miera0% (1)
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument46 pagesCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaNo ratings yet
- Heart Sounds and MurmursDocument38 pagesHeart Sounds and MurmursLaura Moise100% (5)
- CV Review Valvular MurmursDocument9 pagesCV Review Valvular Murmurssiwap34656No ratings yet
- Mitral Stenosis: Ahmad AdityawarmanDocument81 pagesMitral Stenosis: Ahmad AdityawarmanAhmad AdityawarmanNo ratings yet
- Heart Murmurs Topic Review - From Description To AuscultationDocument15 pagesHeart Murmurs Topic Review - From Description To AuscultationRapmle PrasadNo ratings yet
- Approach To Cardiac MurmursDocument11 pagesApproach To Cardiac Murmurstouthang0074085No ratings yet
- Cardio AuscultationDocument19 pagesCardio AuscultationshadabNo ratings yet
- Deskripsi MurmurDocument3 pagesDeskripsi MurmurLevina Tri RatanaNo ratings yet
- Congenital Heart Diseases Practical Approach in Children With Heart MurmurDocument51 pagesCongenital Heart Diseases Practical Approach in Children With Heart Murmurdennyyy175No ratings yet
- Heart MurmursDocument18 pagesHeart MurmursRobby Wiranata WijayaNo ratings yet
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- Heart SoundsDocument56 pagesHeart SoundsBetsy Babilonia100% (1)
- L6) Heart SoundsDocument30 pagesL6) Heart SoundsMar Lar LwinNo ratings yet
- Congenital Heart DiseasesDocument52 pagesCongenital Heart DiseasesCristina Maria100% (1)
- CVS ExaminationDocument72 pagesCVS ExaminationPrashanthBhatNo ratings yet
- Step 1 ShartzDocument333 pagesStep 1 ShartzDaniella Vazquez100% (1)
- Heart Sounds and Arteriovenous Pulses: DR Chandana HewageDocument48 pagesHeart Sounds and Arteriovenous Pulses: DR Chandana HewagePrasad HewawasamNo ratings yet
- Congenital Heart Disease (Part I) : Shenzhou Hospital He LihuiDocument26 pagesCongenital Heart Disease (Part I) : Shenzhou Hospital He LihuiTaran JOt100% (1)
- Cardiovascular System Assessment: Prepared By: Adnan GeorgeDocument40 pagesCardiovascular System Assessment: Prepared By: Adnan GeorgeShah ZamanNo ratings yet
- CVS Examination EditedDocument134 pagesCVS Examination EditedThilak JayalathNo ratings yet
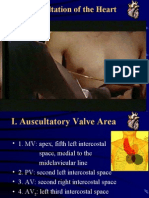
- Cardiac Auscultation: Mark Haigney, MD Mhaigney@usuhs - EduDocument77 pagesCardiac Auscultation: Mark Haigney, MD Mhaigney@usuhs - Eduhüseyin_coşkun_1No ratings yet
- Examination and Investigation of The Cardiovascular System (CVS)Document27 pagesExamination and Investigation of The Cardiovascular System (CVS)Jake MillerNo ratings yet
- Auscultatia CardiacaDocument9 pagesAuscultatia CardiacaMh MhNo ratings yet
- Leaflet Ppds Uns 2018Document32 pagesLeaflet Ppds Uns 2018agungnugoho4247No ratings yet
- CM3 - Cu12 Assessment of Heart & Neck VesselsDocument15 pagesCM3 - Cu12 Assessment of Heart & Neck Vesselseli pascualNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- S and S: Presenter: Guidance and ModerationDocument60 pagesS and S: Presenter: Guidance and ModerationCatherine PaulNo ratings yet
- Chapter (10) : Assessment of Cardiovascular SystemDocument10 pagesChapter (10) : Assessment of Cardiovascular SystemSandra GabasNo ratings yet
- CVS PrecordiumDocument20 pagesCVS PrecordiumSarahNo ratings yet
- Pembekalan Auskultasi Jantung Jimmy AsafDocument45 pagesPembekalan Auskultasi Jantung Jimmy AsafFikriYTNo ratings yet
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- Auscultation of HeartDocument92 pagesAuscultation of Heartsanjivdas100% (1)
- CARDIO PPT Diastolic MurmursDocument47 pagesCARDIO PPT Diastolic MurmursHenry Franz Flores NicolásNo ratings yet
- Cardiovascular ExaminationDocument38 pagesCardiovascular Examinationdrskdcrdio601250% (2)
- Approach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemDocument79 pagesApproach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemLajel S. LachicaNo ratings yet
- JVP and HS .-2Document93 pagesJVP and HS .-2Sahithi ChittepuNo ratings yet
- Cardiac Tamponade: Key Points: Elevated Neck VeinsDocument2 pagesCardiac Tamponade: Key Points: Elevated Neck VeinsPuannita SariNo ratings yet
- PE of Common CVSDocument105 pagesPE of Common CVSKaushal RudaniNo ratings yet
- Extra Systolic Heart SoundDocument23 pagesExtra Systolic Heart SoundAtmaja R. SirupangNo ratings yet
- 07 - 01 - Assessment of Cardiovascular SystemDocument55 pages07 - 01 - Assessment of Cardiovascular SystemSalman Habeeb50% (2)
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Suara Jantung 2Document13 pagesSuara Jantung 2Tesis Maruli Tua SianiparNo ratings yet
- Suara JantungDocument12 pagesSuara JantungTesis Maruli Tua SianiparNo ratings yet
- Rangkuman CCS 1Document16 pagesRangkuman CCS 1Tesis Maruli Tua SianiparNo ratings yet
- Rangkuman CCS 2Document16 pagesRangkuman CCS 2Tesis Maruli Tua SianiparNo ratings yet
- Rangkuman PVCDocument13 pagesRangkuman PVCTesis Maruli Tua SianiparNo ratings yet
- SIRIS 3 DatasheetDocument4 pagesSIRIS 3 DatasheetEdwin AbdurahmanNo ratings yet
- Jntu World: R05 Set No. 2Document8 pagesJntu World: R05 Set No. 2Samiullah MohammedNo ratings yet
- Cipovanje 1.9 JTDDocument6 pagesCipovanje 1.9 JTDmicakojicNo ratings yet
- Problem 1:: DX DX M C KX KX DT DTDocument2 pagesProblem 1:: DX DX M C KX KX DT DTallswellelleNo ratings yet
- Project Zubair Mishrif DGS Expansion Technical Query N. 2510-TQ-C12-ENI-F-0003Document4 pagesProject Zubair Mishrif DGS Expansion Technical Query N. 2510-TQ-C12-ENI-F-0003mangesh patilNo ratings yet
- Butterfly Strategy in Fixed IncomeDocument20 pagesButterfly Strategy in Fixed Incomepaolo lodi100% (1)
- Quick Reference Guide: Important InformationDocument16 pagesQuick Reference Guide: Important InformationDanijela MravikNo ratings yet
- Certene L.A. LLBF-122D (Sustituto 11PG4) ActualizadaDocument1 pageCertene L.A. LLBF-122D (Sustituto 11PG4) ActualizadadianaNo ratings yet
- Daily Lesson Plan Mathematics Year 3Document2 pagesDaily Lesson Plan Mathematics Year 3BrianNo ratings yet
- An Operating Systems Course: With Projects in JavaDocument3 pagesAn Operating Systems Course: With Projects in JavaJonathan JoestarNo ratings yet
- Algebraic ExpressionsDocument17 pagesAlgebraic ExpressionsSkyline MCNo ratings yet
- Degradation of Ibuprofen in Aqueous Solution With UV Light - The Effect of Reactor Volume and PHDocument9 pagesDegradation of Ibuprofen in Aqueous Solution With UV Light - The Effect of Reactor Volume and PHWillonina WhookiNo ratings yet
- General Notes:: Device Id and Symbol Legend ComponentsDocument21 pagesGeneral Notes:: Device Id and Symbol Legend ComponentsVU ingenieriaNo ratings yet
- Analytical Report: PT Sumber Indah PerkasaDocument3 pagesAnalytical Report: PT Sumber Indah PerkasaarisNo ratings yet
- Alloy Steel Round BarDocument10 pagesAlloy Steel Round BarSingarao KattaNo ratings yet
- 8 2 Angle Bisectors of TrianglesDocument8 pages8 2 Angle Bisectors of Trianglesapi-332361871No ratings yet
- Software VerificationDocument28 pagesSoftware VerificationAhmi khanNo ratings yet
- Recurrent Neural Networks by Xiaolin Hu, P. BalasubramaniamDocument410 pagesRecurrent Neural Networks by Xiaolin Hu, P. Balasubramaniamzafar hussainNo ratings yet
- 701 Armox Workshop RecommendationsDocument11 pages701 Armox Workshop RecommendationssudhavelNo ratings yet
- Easy VBADocument93 pagesEasy VBAkham bid100% (1)
- Mazda 3 OBD Codes: EngineDocument13 pagesMazda 3 OBD Codes: EnginecpureaperNo ratings yet
- 02 Data Mining-Partitioning MethodDocument8 pages02 Data Mining-Partitioning MethodRaj EndranNo ratings yet
- DATS3TD2T23BRENDocument11 pagesDATS3TD2T23BRENroa elastal100% (1)
- Lec 1-Machining Operations IIDocument51 pagesLec 1-Machining Operations IIHammad RazaNo ratings yet
- The Use of Remote Sensing in Hydrology PDFDocument260 pagesThe Use of Remote Sensing in Hydrology PDFAngelaFigueroaTapiaNo ratings yet
- 16 - S - 151-1315 - 051 - 141 ZF MenjacDocument65 pages16 - S - 151-1315 - 051 - 141 ZF MenjaczeljkoNo ratings yet