You might also like
- Hammer Toes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHammer Toes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsDocument43 pagesHernia: Inguinal – Surgical anatomy, presentation, treatment, complicationsFobin VargheseNo ratings yet
- Spirometry: Performance and Interpretation A Guide For General PractitionersDocument15 pagesSpirometry: Performance and Interpretation A Guide For General PractitionersAgi AngloSaxonNo ratings yet
- Groin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYDocument39 pagesGroin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYMuhammad Waqar UlfatNo ratings yet
- Mt. Everest QuizDocument17 pagesMt. Everest QuizZanuardi YahyaNo ratings yet
- Hernia - Hernioplasty With Bilayer Polypropylene Mesh PDFDocument4 pagesHernia - Hernioplasty With Bilayer Polypropylene Mesh PDFAnonymous YLmmme4XX0No ratings yet
- Mesh MaterialsDocument21 pagesMesh MaterialsbogdanotiNo ratings yet
- Tension-Free Repair Versus Bassini Technique For SDocument5 pagesTension-Free Repair Versus Bassini Technique For STomus ClaudiuNo ratings yet
- Treatment: Bassini RepairDocument5 pagesTreatment: Bassini RepairziehonkNo ratings yet
- Synchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaDocument6 pagesSynchronous Open Hernioplasty of Primary Bilateral Inguinal HerniaKhaled MonazeaNo ratings yet
- OP Sliding & Strangulated Hernia & OrchiectomyDocument8 pagesOP Sliding & Strangulated Hernia & OrchiectomyDeepika ChaudharyNo ratings yet
- Open Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective StudyDocument3 pagesOpen Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective Study'Adil MuhammadNo ratings yet
- CA OesophagusDocument47 pagesCA OesophagusAnsif KNo ratings yet
- Back To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopDocument43 pagesBack To Basics Fundamentals of Wound Care and Dressing Selection Spring WorkshopBima Achmad100% (1)
- HerniaDocument16 pagesHerniaVetrivel TamizhNo ratings yet
- Premalignant & Malignant Disease of CervixDocument64 pagesPremalignant & Malignant Disease of CervixDegefaw BikoyNo ratings yet
- Motility Disorders of EsophagusDocument44 pagesMotility Disorders of EsophagusmackieccNo ratings yet
- Idiopathic Non Neoplastic Salivary Gland DiseasesDocument33 pagesIdiopathic Non Neoplastic Salivary Gland Diseasesgud4nothingNo ratings yet
- HernioplastyDocument58 pagesHernioplastyFobin VargheseNo ratings yet
- Thyroid Disorders: Types, Symptoms, and TreatmentsDocument41 pagesThyroid Disorders: Types, Symptoms, and Treatmentssheila_kohNo ratings yet
- Etiopathogenesis & Staging of Cancer BreastDocument25 pagesEtiopathogenesis & Staging of Cancer Breastapi-3701915No ratings yet
- SoTM StaplingDocument20 pagesSoTM StaplingIndrawan Buleth100% (1)
- Energy Devices in Surgery: Surg LT CDR K S PatelDocument32 pagesEnergy Devices in Surgery: Surg LT CDR K S PatelMuhammad ShahidNo ratings yet
- Surgical Meshes and Their FixationDocument34 pagesSurgical Meshes and Their FixationShahzad Alam ShahNo ratings yet
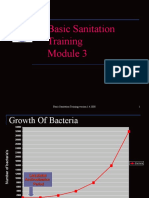
- Basic Sanitation Training Module 3 Version 1 (1) .4.2008Document13 pagesBasic Sanitation Training Module 3 Version 1 (1) .4.2008Chef RoyNo ratings yet
- Principles of Electrosurgery and DiathermyDocument15 pagesPrinciples of Electrosurgery and DiathermyRajarshi KumarNo ratings yet
- Essential Techniques for Safe Thyroid SurgeryDocument26 pagesEssential Techniques for Safe Thyroid SurgeryJimmyNo ratings yet
- Prosthetic Material in Inguinal Hernia RepairDocument23 pagesProsthetic Material in Inguinal Hernia RepairAnca NicaNo ratings yet
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 pagesIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangNo ratings yet
- Diabetic Foot Ulcers Prevention & ManagementDocument59 pagesDiabetic Foot Ulcers Prevention & Managementcharity kalinowsky100% (2)
- Role of neck triangles in identifying structures during thyroid surgeryDocument6 pagesRole of neck triangles in identifying structures during thyroid surgeryJay-arh SebusaNo ratings yet
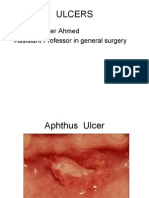
- Ulcer, Cyst, Tumoures, Sinus, FistullaDocument40 pagesUlcer, Cyst, Tumoures, Sinus, Fistulladrhiwaomer100% (2)
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Hernia Examination SchemeDocument4 pagesHernia Examination Schemeatribecalledquest20No ratings yet
- Parotid TumorDocument37 pagesParotid TumorRiyan SaputraNo ratings yet
- Incisional HerniaDocument13 pagesIncisional HerniaMaya Dewi permatasariNo ratings yet
- Abdominal HerniasDocument33 pagesAbdominal Herniastianally100% (2)
- What Is The Differential Diagnosis For The Breast Mass in An Adolescent?Document4 pagesWhat Is The Differential Diagnosis For The Breast Mass in An Adolescent?theodore_estradaNo ratings yet
- Suture and Suturing PDFDocument165 pagesSuture and Suturing PDFcj bariasNo ratings yet
- Herniorrhaphy 1Document60 pagesHerniorrhaphy 1Fobin VargheseNo ratings yet
- Abdominal Trauma Assessment GuideDocument135 pagesAbdominal Trauma Assessment GuidewidyastutiNo ratings yet
- Endometrial Cancer: Manuela RussuDocument38 pagesEndometrial Cancer: Manuela RussuAnonymous 0XqZUl06PmNo ratings yet
- Reconstruction in Fournier GangreneDocument40 pagesReconstruction in Fournier GangreneAnggie MutmainnahNo ratings yet
- Man Age Men T of CancerDocument14 pagesMan Age Men T of CancerKoRnflakesNo ratings yet
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Gen Surgery EssaysDocument161 pagesGen Surgery EssaysВлади ПетковNo ratings yet
- Assessing AbdomenDocument115 pagesAssessing AbdomenKris TinaNo ratings yet
- Management of Acute and Chronic Urinary RetentionDocument52 pagesManagement of Acute and Chronic Urinary RetentionSri HariNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- Wound Documentation Tips PDFDocument2 pagesWound Documentation Tips PDFWinnie LiNo ratings yet
- Varicose Veins CaseDocument16 pagesVaricose Veins Casebenak shivalingappaNo ratings yet
- Penetrating Trauma ManagementDocument103 pagesPenetrating Trauma ManagementAlrexan B. MalatagNo ratings yet
- Amputation in Lower LimbsDocument35 pagesAmputation in Lower LimbsSamNo ratings yet
- (DERMA) 03 TineasDocument9 pages(DERMA) 03 TineasJolaine ValloNo ratings yet
- I Flat Meshes For Inguinal and Ventral Hernias V 2Document30 pagesI Flat Meshes For Inguinal and Ventral Hernias V 2bogdanoti100% (1)
- The Surgical Anatomy of The Nerve Laryngeal RecurrensDocument2 pagesThe Surgical Anatomy of The Nerve Laryngeal RecurrensvaNo ratings yet
- Disorders of Parathyroid Glands: Hyperparathyroidism and HypoparathyroidismDocument52 pagesDisorders of Parathyroid Glands: Hyperparathyroidism and HypoparathyroidismDr. Akash GuptaNo ratings yet
- WOUND HEALING: THE 3 STAGES AND COMPLICATIONSDocument21 pagesWOUND HEALING: THE 3 STAGES AND COMPLICATIONSOsama Fadel ahmedNo ratings yet
- TYT DM UVF10 Programming Guide v1.0 PDFDocument48 pagesTYT DM UVF10 Programming Guide v1.0 PDFCesar Del CastilloNo ratings yet
- HERNIADocument70 pagesHERNIAmwro789000No ratings yet
- Sop For FatDocument6 pagesSop For Fatahmed ismailNo ratings yet
- Quality Control and Quality AssuranceDocument7 pagesQuality Control and Quality AssuranceMoeen Khan Risaldar100% (1)
- Chapter 11 RespirationDocument2 pagesChapter 11 Respirationlock_jaw30No ratings yet
- My Demo DemoDocument19 pagesMy Demo DemoAlex LopezNo ratings yet
- Chapter 24 Study QuestionsDocument3 pagesChapter 24 Study QuestionsAline de OliveiraNo ratings yet
- Javelin Mobility Ability 2.0 GuideDocument36 pagesJavelin Mobility Ability 2.0 Guideroham25156No ratings yet
- Leaving Cert Maths ScholarshipsDocument3 pagesLeaving Cert Maths ScholarshipsJohn HayesNo ratings yet
- Islamic Center Design With Islamic ArchiDocument11 pagesIslamic Center Design With Islamic ArchiMuhammad Sufiyan SharafudeenNo ratings yet
- COVID-19 and Flu Vaccination Walgreens Immunization ServicesDocument1 pageCOVID-19 and Flu Vaccination Walgreens Immunization ServicesAitana MaldonadoNo ratings yet
- Titan InvoiceDocument1 pageTitan Invoiceiamdhanush017No ratings yet
- Advanced Guide To Digital MarketingDocument43 pagesAdvanced Guide To Digital MarketingArpan KarNo ratings yet
- I3rc Insights Pvt. Ltd. India - Company Credentials PDFDocument28 pagesI3rc Insights Pvt. Ltd. India - Company Credentials PDFManoj Kumar JhaNo ratings yet
- Role of Therapeutic Gardens in Healthy Cities: Design StandardsDocument3 pagesRole of Therapeutic Gardens in Healthy Cities: Design Standardsaarthi SureshNo ratings yet
- 2019 Indonesia Salary GuideDocument32 pages2019 Indonesia Salary Guideiman100% (1)
- DissertationDocument15 pagesDissertationNicole BradyNo ratings yet
- Pruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Document2 pagesPruebas de Certificación Lingüística in - B1 - Ce - Sol - J - 2015 Answer Key - JUNE 2015 Task 1Jeru SierraNo ratings yet
- CBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and SaltsDocument11 pagesCBSE Class 10 Science Revision Notes Chapter - 2 Acids, Bases and Saltsmilind dhamaniyaNo ratings yet
- G.raju Reddy Resume (PDF1) PDFDocument3 pagesG.raju Reddy Resume (PDF1) PDFanon_708469687No ratings yet
- Master in Public Management: Application PacketDocument6 pagesMaster in Public Management: Application PacketMark GironNo ratings yet
- Gigabyte 8simlh - Rev 3.02Document32 pagesGigabyte 8simlh - Rev 3.02Denis MartinsNo ratings yet
- 25 Mosquito Facts and TriviaDocument3 pages25 Mosquito Facts and Triviamara_hahaNo ratings yet
- Goethe Zertifikat b1 HorenDocument2 pagesGoethe Zertifikat b1 HorenLevent75% (4)
- My CV - Rose ChebetDocument5 pagesMy CV - Rose ChebetSammy WatimaNo ratings yet
- Direct Marketing: Mcgraw-Hill/IrwinDocument30 pagesDirect Marketing: Mcgraw-Hill/IrwinJunaid KhalidNo ratings yet
- Summary G.E 9 Rizal Works (Chapter 1-13)Document23 pagesSummary G.E 9 Rizal Works (Chapter 1-13)Erwin Jay CabantacNo ratings yet
- Edited Hydraulics Lecture - Part 2 - OrificesDocument36 pagesEdited Hydraulics Lecture - Part 2 - OrificesVincentNo ratings yet
- A Beginners Guide Sap Smart FormsDocument61 pagesA Beginners Guide Sap Smart FormsMuhammad ZeeshanNo ratings yet
- Guidelines SLCM BWDocument60 pagesGuidelines SLCM BWpnaarayanNo ratings yet
- Integrated Marketing Communication PlanDocument5 pagesIntegrated Marketing Communication Planprojectwork185No ratings yet
- RRT LH: Gt'R:Ut (TLDocument75 pagesRRT LH: Gt'R:Ut (TLkl equipmentNo ratings yet