You might also like
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Presented By: Raghav Dogra M.Pharm (Analysis) 2016-2017Document38 pagesPresented By: Raghav Dogra M.Pharm (Analysis) 2016-2017gggNo ratings yet
- Drugs Interactions May 2010Document28 pagesDrugs Interactions May 2010Michael MohammedNo ratings yet
- An Introduction to Mechanisms in Pharmacology and TherapeuticsFrom EverandAn Introduction to Mechanisms in Pharmacology and TherapeuticsNo ratings yet
- DRUG INTERACTIONS: CLASSIFICATION AND PRINCIPLESDocument40 pagesDRUG INTERACTIONS: CLASSIFICATION AND PRINCIPLESAbdalla Kazzam100% (1)
- Drug & Therapeutic InteractionsDocument28 pagesDrug & Therapeutic Interactionsفاطمة الجش.No ratings yet
- Drug InteractionDocument77 pagesDrug InteractionAthirah Muhammad NoerNo ratings yet
- Drug InteractionDocument26 pagesDrug InteractionABDURRAHMAN ASY-SYAKUUR 1No ratings yet
- Drug InteractionDocument20 pagesDrug InteractionRajendra Moorthy RajendranNo ratings yet
- Drug Drug Interactions 2Document133 pagesDrug Drug Interactions 2joo saadNo ratings yet
- Sunitha - Drug InteractionsDocument49 pagesSunitha - Drug InteractionsSunitha Katta100% (1)
- Pharmacokinetic Drug InteractionsDocument3 pagesPharmacokinetic Drug InteractionsRaghu RamarapuNo ratings yet
- PharmaDocument21 pagesPharmaChalbi Marie FernandezNo ratings yet
- Drug Interaction SourcesDocument5 pagesDrug Interaction Sourcesvajkember100% (1)
- CU SHAH - Refresher Course - 02-10-2016 FinalDocument38 pagesCU SHAH - Refresher Course - 02-10-2016 FinalParthMairNo ratings yet
- Pharmacokinetic Drug Interactions: Narendra. B 2010H146035HDocument40 pagesPharmacokinetic Drug Interactions: Narendra. B 2010H146035HNarendra BhupatiNo ratings yet
- Drug Interactions With Tuberculosis TherapyDocument5 pagesDrug Interactions With Tuberculosis TherapypriyankaNo ratings yet
- Drug InteractionsDocument19 pagesDrug InteractionsMehveen KashifNo ratings yet
- IVMS Pharmacokinetics Drug Elimination 2Document33 pagesIVMS Pharmacokinetics Drug Elimination 2piinyNo ratings yet
- Mid Human Pharma 23-24Document6 pagesMid Human Pharma 23-24Linh NguyễnNo ratings yet
- Drug InteractonsDocument32 pagesDrug InteractonsHarun MohamedNo ratings yet
- Drug InteractionDocument151 pagesDrug Interactionapi-3724213100% (1)
- Drug Interactions ExplainedDocument147 pagesDrug Interactions ExplainedSandhy TampubolonNo ratings yet
- 1 Drug Interaction Spring 2024Document68 pages1 Drug Interaction Spring 2024192315No ratings yet
- Drug Interaction Can Be Defined As TheDocument34 pagesDrug Interaction Can Be Defined As TheIstianah Es100% (1)
- Unit-2 Drug InteractionsDocument29 pagesUnit-2 Drug InteractionsMohammad Kaif50% (2)
- Drug InteractionsDocument43 pagesDrug InteractionsNinaNo ratings yet
- Drug Interactions: Vivian Soetikno Department of Pharmacology & Therapeutics, FmuiDocument53 pagesDrug Interactions: Vivian Soetikno Department of Pharmacology & Therapeutics, FmuiAciNo ratings yet
- General PHARMACOLOGYDocument17 pagesGeneral PHARMACOLOGYAndreNo ratings yet
- DRUG Interactions by Dr. HadiaDocument30 pagesDRUG Interactions by Dr. HadiaDr. Hadia NadeemNo ratings yet
- Interaksi ObatDocument37 pagesInteraksi ObatYustia SariNo ratings yet
- Drug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019Document32 pagesDrug Interactions: DR Michelle Munyoro MBCHB, MCPH (Uz) 6 February 2019Stanley Tatenda MukonoNo ratings yet
- Drug InteractionDocument23 pagesDrug Interactionsinghjsanjay885No ratings yet
- Drug Interaction Can Be Defined As TheDocument34 pagesDrug Interaction Can Be Defined As TheBhavana GangurdeNo ratings yet
- DRUG INTERACTIONS: MECHANISMS AND PREVENTIONDocument21 pagesDRUG INTERACTIONS: MECHANISMS AND PREVENTIONكسلان اكتب اسميNo ratings yet
- 2.5. Drugs Interaction (Dr. Kinanti)Document135 pages2.5. Drugs Interaction (Dr. Kinanti)dikri pangersaNo ratings yet
- Drug InteractionDocument27 pagesDrug InteractionRida Nur RafidahNo ratings yet
- Drug Interactions: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDocument28 pagesDrug Interactions: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDigvijayaNo ratings yet
- DruginteractionDocument28 pagesDruginteractionसन्दिप क्षेत्रीNo ratings yet
- Pharmacokinetics and Drug DistributionDocument6 pagesPharmacokinetics and Drug DistributionRumana ShaikhNo ratings yet
- Drug Interactions: Endang Windiastuti, Dr.,Spa (K) Satgas Farmasi IdaiDocument30 pagesDrug Interactions: Endang Windiastuti, Dr.,Spa (K) Satgas Farmasi IdaiFredik MaloNo ratings yet
- INteraksi Obat IIDocument16 pagesINteraksi Obat IIpatimah simamoraNo ratings yet
- 1 PB PDFDocument5 pages1 PB PDFAlkaustariyah LubisNo ratings yet
- Drug Drug InteractionDocument9 pagesDrug Drug InteractionB.pharm 16th BatchNo ratings yet
- Drug InteractionsDocument46 pagesDrug InteractionsAvinash Chaudhary100% (1)
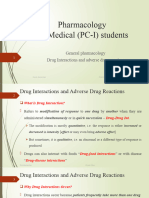
- Drug Interaction and Adverse Drug Interactions PCI StudentsDocument38 pagesDrug Interaction and Adverse Drug Interactions PCI Studentsabdijorgi1No ratings yet
- Drug InteractionsDocument33 pagesDrug Interactions88AKK100% (1)
- 1 PBDocument8 pages1 PBTaulant SalihuNo ratings yet
- Pharmacokinetic Interaction: DR - Datten Bangun MSC, SPFK & DR - Zulkarnain RangkutyDocument39 pagesPharmacokinetic Interaction: DR - Datten Bangun MSC, SPFK & DR - Zulkarnain RangkutyCatherine ElizabetNo ratings yet
- Drug - Drug Int2Document35 pagesDrug - Drug Int2alishba100% (2)
- Drug-Drug-Gene Interactions and PharmacogeneticsDocument26 pagesDrug-Drug-Gene Interactions and PharmacogeneticsMarfu'ah Mar'ahNo ratings yet
- Naveen Kumar.M M.Pharmacy (Pharmaceutics) - 10Y81SO310Document29 pagesNaveen Kumar.M M.Pharmacy (Pharmaceutics) - 10Y81SO310Benish RasheedNo ratings yet
- Drug InteractionsDocument30 pagesDrug InteractionsmikhaelyosiaNo ratings yet
- DRUG INTERACTION MECHANISMSDocument42 pagesDRUG INTERACTION MECHANISMSVanita ValluvanNo ratings yet
- Clinically Relevant Drug-Drug Interactions in Oncology: Howard L. McleodDocument6 pagesClinically Relevant Drug-Drug Interactions in Oncology: Howard L. McleodCindyGaniNo ratings yet
- Drug Interactions: MSC Tid 1 Nyakundi BM April 21 2010Document43 pagesDrug Interactions: MSC Tid 1 Nyakundi BM April 21 2010MONALISA MISTRINo ratings yet
- Interaksi FarmakokinetikDocument43 pagesInteraksi FarmakokinetikGarry B GunawanNo ratings yet
- Lecture 3Document12 pagesLecture 3ahmedfawakh0No ratings yet
- Prepared By: Anoosha Samma Sawera HibaDocument12 pagesPrepared By: Anoosha Samma Sawera HibaAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument8 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Drug Induced Hematological DisordersDocument49 pagesDrug Induced Hematological DisordersAnoosha FarooquiNo ratings yet
- Safety Measures in Pharmaaceutical IndustryDocument1 pageSafety Measures in Pharmaaceutical IndustryAnoosha FarooquiNo ratings yet
- Anoosha Farooqui 2 Year (4 Semester) Pharmacy 501-S19-001 Bio-Statistics Pharm 419 3 Sir MasoodDocument1 pageAnoosha Farooqui 2 Year (4 Semester) Pharmacy 501-S19-001 Bio-Statistics Pharm 419 3 Sir MasoodAnoosha FarooquiNo ratings yet
- Column Chromatography ExplainedDocument4 pagesColumn Chromatography ExplainedAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Computer Applications in Community PharmacyDocument9 pagesComputer Applications in Community PharmacyAnoosha FarooquiNo ratings yet
- Community PharmacyDocument5 pagesCommunity PharmacyAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument8 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of SubmissionDocument10 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of SubmissionAnoosha FarooquiNo ratings yet
- Anoosha Farooqui 3 Year (5 Semester) Pharmacy 501-S19-001 Pathology PHARM 514 3+1 Miss Noreen 2 February 2021 10 February 2021Document2 pagesAnoosha Farooqui 3 Year (5 Semester) Pharmacy 501-S19-001 Pathology PHARM 514 3+1 Miss Noreen 2 February 2021 10 February 2021Anoosha FarooquiNo ratings yet
- Group 07 Report on Extemporaneous Powder DispensingDocument7 pagesGroup 07 Report on Extemporaneous Powder DispensingAnoosha FarooquiNo ratings yet
- Tablets and CapsuleDocument23 pagesTablets and CapsuleAnoosha FarooquiNo ratings yet
- Evaluation of DrugsDocument11 pagesEvaluation of DrugsAnoosha FarooquiNo ratings yet
- GingerDocument3 pagesGingerAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Assignment of QCMDocument14 pagesAssignment of QCMAnoosha FarooquiNo ratings yet
- Oral Hygiene ProductsDocument20 pagesOral Hygiene ProductsAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Islamiat AssignmentDocument11 pagesIslamiat AssignmentAnoosha FarooquiNo ratings yet
- Evaluation of DrugsDocument11 pagesEvaluation of DrugsAnoosha FarooquiNo ratings yet
- SUSPENSIONDocument11 pagesSUSPENSIONAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument2 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Clinical Guideline For Anticoagulant Use in AdultsDocument108 pagesClinical Guideline For Anticoagulant Use in Adultsmonday125No ratings yet
- 109 Questions and Rationale On Psychotic Disorders IIIDocument32 pages109 Questions and Rationale On Psychotic Disorders IIIChaelo SantosNo ratings yet
- CB TheFearfulAnxiousWorriedPet - Solliquin.DePorter11.2015Document5 pagesCB TheFearfulAnxiousWorriedPet - Solliquin.DePorter11.2015Anonymous TDI8qdYNo ratings yet
- Assignment - Headache DisordersDocument2 pagesAssignment - Headache DisordersAyessa SalazarNo ratings yet
- Diary Retail (AutoRecovered)Document56 pagesDiary Retail (AutoRecovered)Maizurah ZulkafliNo ratings yet
- 2022 ISPAD Clinical Practice Consensus Guidelines 2022Document70 pages2022 ISPAD Clinical Practice Consensus Guidelines 2022WenSarmientoBNo ratings yet
- G.glabra FullDocument7 pagesG.glabra FullSiva PrasadNo ratings yet
- Foundation of Professional Nursing Practice Review (40Document25 pagesFoundation of Professional Nursing Practice Review (40Sittie Haya LazimNo ratings yet
- Regulation5362014 Qa enDocument143 pagesRegulation5362014 Qa enmeiNo ratings yet
- EAT what you can EVALUATE and ASSESS; TEACH the restDocument43 pagesEAT what you can EVALUATE and ASSESS; TEACH the restJessie LendioNo ratings yet
- Preparation and Evaluation of Sustained Release Aminophylline TabletDocument10 pagesPreparation and Evaluation of Sustained Release Aminophylline TabletardiNo ratings yet
- 2.C. Laporan Penyimpanan ObatDocument9 pages2.C. Laporan Penyimpanan ObatNovi AstutiNo ratings yet
- Management of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerDocument10 pagesManagement of Local Anesthetic Complications: Ross Camiel, Samuel Roh, and Christy LottingerErryskaNo ratings yet
- Nyoba Bikin AplikasiDocument6 pagesNyoba Bikin Aplikasiperdana aris kusumaNo ratings yet
- Cisplatin dosage, side effects, and nursing responsibilitiesDocument1 pageCisplatin dosage, side effects, and nursing responsibilitieskyawNo ratings yet
- Clarisse B. Cerame - Drug Study - PsychopharmacologyDocument5 pagesClarisse B. Cerame - Drug Study - PsychopharmacologyClarisse Biagtan CerameNo ratings yet
- Case Study Hypertension: Name: Jay Villasoto Bsn-3 StemDocument28 pagesCase Study Hypertension: Name: Jay Villasoto Bsn-3 StemJay VillasotoNo ratings yet
- Medicin All Nov, Sep, OctDocument98 pagesMedicin All Nov, Sep, OctMohammad BanisalmanNo ratings yet
- Central Nervous System MedicationsDocument12 pagesCentral Nervous System MedicationsMARY JEANINA ALBANo ratings yet
- Shawan Pharma Equipment SOPsDocument47 pagesShawan Pharma Equipment SOPsdaizhussain004100% (1)
- Martindale 40 - 9780857113672 PDFDocument1 pageMartindale 40 - 9780857113672 PDFNatanaela60% (5)
- Efficacy of Caffeine in Promoting Hair Growth by Enhancing Intracellular Activity of Hair FolliclesDocument8 pagesEfficacy of Caffeine in Promoting Hair Growth by Enhancing Intracellular Activity of Hair FolliclesElsayed Refaat Aly MareyNo ratings yet
- Aromatherapy Massage For Neuro PDFDocument11 pagesAromatherapy Massage For Neuro PDFTitin JuherniNo ratings yet
- Antalox PI - Group 8Document3 pagesAntalox PI - Group 8Alyssa Nicole PadillaNo ratings yet
- Physiology AnsDocument25 pagesPhysiology Ansshalialoo22100% (1)
- Hormone Therapy For Prostate CancerDocument10 pagesHormone Therapy For Prostate CancerChrisNo ratings yet
- Pharmacology Assignment: Student's NameDocument6 pagesPharmacology Assignment: Student's NameMosesNo ratings yet
- Cerebral CirculationDocument25 pagesCerebral Circulation20AR018 HARIHARA SUBRAMANIANNo ratings yet
- Radioimmunoassay Enzyme and Non-enzyme-Based ImmunDocument5 pagesRadioimmunoassay Enzyme and Non-enzyme-Based ImmunTaqua SeamNo ratings yet
- Registered Medicine List 07-04-2014 Sse Frequently UpdatedDocument116 pagesRegistered Medicine List 07-04-2014 Sse Frequently Updatedjema; belihuNo ratings yet