You might also like
- Littelfuse EVI EV Charging Infrastructure Presentation PDFDocument19 pagesLittelfuse EVI EV Charging Infrastructure Presentation PDFRaka Pratindy100% (1)
- De My Eli NationDocument7 pagesDe My Eli NationGeorge ForțuNo ratings yet
- Demyelinating Disorders: Prof. DRDocument51 pagesDemyelinating Disorders: Prof. DRKhaled OssamaNo ratings yet
- W3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Document11 pagesW3 - MEDSURG Neurologic Disorders (MS, MG, and Parkisons's)Kyla L. MadjadNo ratings yet
- Cerebellar Disorders: Dr. Mohamed Nasreldin HamdoonDocument14 pagesCerebellar Disorders: Dr. Mohamed Nasreldin HamdoonMohamed Nasreldin HamdoonNo ratings yet
- c4f - Multiple SclerosisDocument240 pagesc4f - Multiple Sclerosisstewpitt2No ratings yet
- A Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosisDocument7 pagesA Serum Autoantibody Marker of Neuromyelitis Optica: Distinction From Multiple SclerosistiaraleshaNo ratings yet
- Pediatrics Concept BookDocument312 pagesPediatrics Concept Bookram dheerNo ratings yet
- 1926 PapionianDocument108 pages1926 PapionianPLCS_FoundationNo ratings yet
- Zombieworld PlaytestDocument30 pagesZombieworld PlaytestWellameGranaNo ratings yet
- Cisco 1 Reviewer For Final ExamDocument9 pagesCisco 1 Reviewer For Final ExamAlNo ratings yet
- Brain TumorsDocument19 pagesBrain TumorsNavjot BrarNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Basic SCBA: Self-Contained Breathing ApparatusDocument51 pagesBasic SCBA: Self-Contained Breathing ApparatusPaoloFregonaraNo ratings yet
- Austin Journal of Multiple Sclerosis & NeuroimmunologyDocument14 pagesAustin Journal of Multiple Sclerosis & NeuroimmunologyAustin Publishing GroupNo ratings yet
- Practice Writing Effective SentencesDocument5 pagesPractice Writing Effective SentencesHaekal FarabyNo ratings yet
- The Spectrum of Neuromyelitis Optica: ReviewDocument11 pagesThe Spectrum of Neuromyelitis Optica: ReviewRiccardo TroiaNo ratings yet
- Listeria Monocytogenes Guidance On: Environmental Monitoring and Corrective Actions in At-Risk FoodsDocument35 pagesListeria Monocytogenes Guidance On: Environmental Monitoring and Corrective Actions in At-Risk FoodsGaganpreet KaurNo ratings yet
- UMNLand AHCDocument27 pagesUMNLand AHCdrmamodoNo ratings yet
- Neurofibromatosis - Pediatrics - MSD Manual Professional EditionDocument8 pagesNeurofibromatosis - Pediatrics - MSD Manual Professional Editioncynthiadamayanti_drNo ratings yet
- Neurologicemergenciesin Pediatricpatients Includingaccidentaland NonaccidentaltraumaDocument18 pagesNeurologicemergenciesin Pediatricpatients Includingaccidentaland NonaccidentaltraumaAvrilMontNo ratings yet
- Multiple SclerosisDocument91 pagesMultiple SclerosisAaron James GrayNo ratings yet
- Demyelinating Diseases: My ApproachDocument9 pagesDemyelinating Diseases: My ApproachRyana Fitriana IINo ratings yet
- Referat Genomics Brain TumorDocument51 pagesReferat Genomics Brain TumorAlessia Wyneini TirzaNo ratings yet
- Moyamoya DiseaseDocument12 pagesMoyamoya DiseaseFarida Irawati SiregarNo ratings yet
- Approach To Fetal Anomalies 2022Document52 pagesApproach To Fetal Anomalies 2022Mohammad AlrefaiNo ratings yet
- 1) Tay-Sachs Disease & Lysosomes: Elizabeth Jade Vicera 3bio1Document2 pages1) Tay-Sachs Disease & Lysosomes: Elizabeth Jade Vicera 3bio1Beatrix MedinaNo ratings yet
- Multiple SclerosisDocument14 pagesMultiple Sclerosisbrianpeterson000No ratings yet
- Multiple Sclerosis RevalidaDocument8 pagesMultiple Sclerosis RevalidaMarielle RamesoNo ratings yet
- Song 2016Document19 pagesSong 2016MarwanNo ratings yet
- Brain Tumors: ReviewDocument9 pagesBrain Tumors: ReviewsarabisimonaNo ratings yet
- 5 MSDocument37 pages5 MSKim GonzalesNo ratings yet
- Deg ModuleDocument15 pagesDeg Modulebiswajitpaul8403No ratings yet
- Biopsych Reviewer For FinalsDocument6 pagesBiopsych Reviewer For Finalsnicole.recedeNo ratings yet
- Nejmra 1904655Document9 pagesNejmra 1904655silviaNo ratings yet
- SyndromesDocument19 pagesSyndromesapi-26826496No ratings yet
- On Demand Pediatric SkullDocument20 pagesOn Demand Pediatric SkullMalekseuofi مالك السيوفيNo ratings yet
- Multiple Sclerosis 1.1. Definition: Immunologic DisorderDocument21 pagesMultiple Sclerosis 1.1. Definition: Immunologic Disordergrazelantonette.calubNo ratings yet
- Neurofibromatosis: Dr. SRI HASTUTI, SP.S (K) KSM Neurologi FK Unsyiah/Rsudza 2019Document11 pagesNeurofibromatosis: Dr. SRI HASTUTI, SP.S (K) KSM Neurologi FK Unsyiah/Rsudza 2019Afifah NaurahNo ratings yet
- Brain Tumours: Incidence, Survival, and Aetiology: P A MckinneyDocument6 pagesBrain Tumours: Incidence, Survival, and Aetiology: P A MckinneySaman VithanageNo ratings yet
- The Spectrum of Neuromyelitis Optica: ReviewDocument11 pagesThe Spectrum of Neuromyelitis Optica: ReviewMonica Aleja FernándezNo ratings yet
- Facial PalsyDocument25 pagesFacial PalsyMahad abuukarNo ratings yet
- 2.lab Systemic Path CNS Exercise NeucomDocument6 pages2.lab Systemic Path CNS Exercise NeucomElysa Dela CruzNo ratings yet
- Multiple SclerosisDocument2 pagesMultiple SclerosisAnithamol BabuNo ratings yet
- Multiple Sclerosis: Paola Viñé OrtegaDocument21 pagesMultiple Sclerosis: Paola Viñé OrtegaPaola ViñéNo ratings yet
- Espectro Neuromielitis Óptica 2022 NejmDocument9 pagesEspectro Neuromielitis Óptica 2022 NejmOscar BushNo ratings yet
- Clinically Isolated Syndrome (CIS)Document12 pagesClinically Isolated Syndrome (CIS)Dorin Cristian AntalNo ratings yet
- 2 5291964174748882717Document11 pages2 5291964174748882717نشط عقلكNo ratings yet
- Acute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional Edition PDFDocument3 pagesAcute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional Edition PDFcrsscribdNo ratings yet
- Acute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional EditionDocument3 pagesAcute Transverse Myelitis - Neurologic Disorders - MSD Manual Professional EditioncrsscribdNo ratings yet
- Variants of Multiple Sclerosis: Jack H. Simon,, B.K. Kleinschmidt-DemastersDocument14 pagesVariants of Multiple Sclerosis: Jack H. Simon,, B.K. Kleinschmidt-DemastersNoor HadiNo ratings yet
- Mcfaline Figueroa2018Document9 pagesMcfaline Figueroa2018Kang LimbaNo ratings yet
- Brain & Spinal Cord Tumor: Miss.S.Krishana Lecturer (Prob) SHS, FHCS, EuslDocument24 pagesBrain & Spinal Cord Tumor: Miss.S.Krishana Lecturer (Prob) SHS, FHCS, EuslSalman SalmanNo ratings yet
- Inflammatory DisordersDocument4 pagesInflammatory DisordersArouetNo ratings yet
- Multiple SclerosisDocument10 pagesMultiple SclerosisShefali SharmaNo ratings yet
- Pdf4-Cellabb-brain and Nervous System CancerDocument10 pagesPdf4-Cellabb-brain and Nervous System CancerGRACIAN JOLES BESINNo ratings yet
- Powers1996 Article PathologyOfMyelinDocument8 pagesPowers1996 Article PathologyOfMyelinMahmoud AbouelsoudNo ratings yet
- Nejmra1904794 MDSDDocument17 pagesNejmra1904794 MDSDRolando QuirozNo ratings yet
- 016penyakit DemielinisasiDocument12 pages016penyakit DemielinisasiMuhamad Azrul AwalludinNo ratings yet
- Progressive MyopathyDocument56 pagesProgressive MyopathySnezana MihajlovicNo ratings yet
- 1073 FullDocument7 pages1073 FullMaria Esther GomezNo ratings yet
- Arch Dis Child 2003 Stonehouse 122 4Document4 pagesArch Dis Child 2003 Stonehouse 122 4carlaNo ratings yet
- Recognizing, Diagnosing, and Treating Mitochondrial DiseaseDocument57 pagesRecognizing, Diagnosing, and Treating Mitochondrial DiseaseSnezana MihajlovicNo ratings yet
- EncephalitisDocument17 pagesEncephalitiseko andryNo ratings yet
- The Diferential Diagnosis of MS - JNNP 2001Document7 pagesThe Diferential Diagnosis of MS - JNNP 2001Filipe Gustavo LopesNo ratings yet
- Path Prep - GeoffDocument98 pagesPath Prep - GeoffVerlyn YtNo ratings yet
- 10 1056@NEJMra1904794 PDFDocument17 pages10 1056@NEJMra1904794 PDFMартин ДончевNo ratings yet
- Behavioral Neurology Series: by Mohamed Nasreldin Hamdoon Ass. Professor of Neurology - Sohag UniversityDocument76 pagesBehavioral Neurology Series: by Mohamed Nasreldin Hamdoon Ass. Professor of Neurology - Sohag UniversityMohamed Nasreldin HamdoonNo ratings yet
- Movement Disorders: DR/ Mohamed Nasreldin Hamdoon Ass. Professor of Neurology Sohag University EgyptDocument26 pagesMovement Disorders: DR/ Mohamed Nasreldin Hamdoon Ass. Professor of Neurology Sohag University EgyptMohamed Nasreldin HamdoonNo ratings yet
- Brain OdemaDocument2 pagesBrain OdemaMohamed Nasreldin HamdoonNo ratings yet
- A 388 - A 388M - 03 - Qtm4oc9bmzg4tqDocument8 pagesA 388 - A 388M - 03 - Qtm4oc9bmzg4tqRod RoperNo ratings yet
- Montague Street Cable Car, Wall Street FerryDocument23 pagesMontague Street Cable Car, Wall Street FerryBob DiamondNo ratings yet
- Numerical WindingDocument12 pagesNumerical Windingsujal jhaNo ratings yet
- 10069-9-V01-Ef00-00039 Fire Alarm SystemDocument49 pages10069-9-V01-Ef00-00039 Fire Alarm Systemahffg nnffNo ratings yet
- Measure Guide Air Cond DiagnosticsDocument70 pagesMeasure Guide Air Cond Diagnosticsayad60No ratings yet
- Police Log July 30, 2016Document16 pagesPolice Log July 30, 2016MansfieldMAPoliceNo ratings yet
- Tecnical Data TYPE 139 L12R / L16RDocument1 pageTecnical Data TYPE 139 L12R / L16RLada LabusNo ratings yet
- Bubble Slabs Burned at 800 °C With Different Periods: IOP Conference Series: Materials Science and EngineeringDocument10 pagesBubble Slabs Burned at 800 °C With Different Periods: IOP Conference Series: Materials Science and Engineeringshilpa jacobNo ratings yet
- EmpathyDocument5 pagesEmpathyHijaab KhaanNo ratings yet
- Spesifikasi Vista 120 S Patient Monitor - StandardDocument2 pagesSpesifikasi Vista 120 S Patient Monitor - StandardHadi AtmojoNo ratings yet
- Manual HB ISM112 EDocument106 pagesManual HB ISM112 EALFAKNo ratings yet
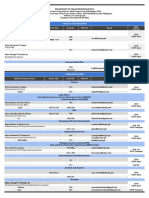
- Updated DOTr Directory As of 29 October 2021Document9 pagesUpdated DOTr Directory As of 29 October 2021Twinkle MiguelNo ratings yet
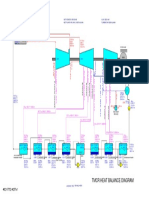
- 01 TMCR Heat Balance DiagramDocument1 page01 TMCR Heat Balance DiagramPrescila PalacioNo ratings yet
- J-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekDocument9 pagesJ-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekMahesNo ratings yet
- 22.anaerobes (Part II)Document91 pages22.anaerobes (Part II)sigrid jaramilloNo ratings yet
- CSCI101 - Lab08 - Functions Zewail CityDocument4 pagesCSCI101 - Lab08 - Functions Zewail CityMahmoud Ahmed 202201238No ratings yet
- E TIMA News Letter November 2016 2 Min - CompressedDocument39 pagesE TIMA News Letter November 2016 2 Min - Compressedasidique5_292665351No ratings yet
- Class XL (The Portrait of A Lady)Document7 pagesClass XL (The Portrait of A Lady)tmoNo ratings yet
- 4K Resolution: The Future of ResolutionsDocument15 pages4K Resolution: The Future of ResolutionsRavi JoshiNo ratings yet
- Determination of Boiling Range Distribution of Crude Petroleum by Gas ChromatographyDocument7 pagesDetermination of Boiling Range Distribution of Crude Petroleum by Gas ChromatographyahmedNo ratings yet
- Freight ForwardingDocument43 pagesFreight ForwardingEuroline NtombouNo ratings yet
- Construction and Building Materials: Paolo ForaboschiDocument21 pagesConstruction and Building Materials: Paolo ForaboschiMarco CamposNo ratings yet