You might also like
- A Simple Guide to Meniscus with Acl Injury, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Meniscus with Acl Injury, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ankle ComplexDocument95 pagesAnkle ComplexMangala Prema MohanarangamNo ratings yet
- Kinesiology Ankle and Foot WULDocument46 pagesKinesiology Ankle and Foot WULwulandari pramanaNo ratings yet
- The Ankle Joint: Articulating BonesDocument5 pagesThe Ankle Joint: Articulating BonesJoe SpencerNo ratings yet
- Ankle Foot BiomechanicsDocument38 pagesAnkle Foot BiomechanicsAnish BishwakarmaNo ratings yet
- Knee Biomechanics: Andrew CrosbyDocument32 pagesKnee Biomechanics: Andrew CrosbyBhanu Pratap PangteyNo ratings yet
- Lecture 1 Knee OrthosesDocument50 pagesLecture 1 Knee OrthosesAlfred JacksonNo ratings yet
- ANATOMY AND BIOMECHANICS OF WRIST JOINT FinalDocument43 pagesANATOMY AND BIOMECHANICS OF WRIST JOINT Finalinas ismailNo ratings yet
- Ankle Anatomy and Blood Supply of TalusDocument66 pagesAnkle Anatomy and Blood Supply of TalusShashank29 LakkalaNo ratings yet
- Ankle Sprain Rehabilitation ProtocolDocument3 pagesAnkle Sprain Rehabilitation ProtocolMuhammad Luqmanulhakim Abu BakarNo ratings yet
- Biomechanics BHIP JOINTDocument68 pagesBiomechanics BHIP JOINTLinmayee SamalNo ratings yet
- Archs of The Foot - May 023Document33 pagesArchs of The Foot - May 023mrizvi334No ratings yet
- Surgical Incisions of Lower LimbDocument11 pagesSurgical Incisions of Lower LimbcpradheepNo ratings yet
- Shoulder Arthroscopy Patient Education Packet RayappaDocument5 pagesShoulder Arthroscopy Patient Education Packet Rayappaapi-549337910No ratings yet
- Lateral Ankel InstabilityDocument16 pagesLateral Ankel InstabilityAleCsss123No ratings yet
- Vivek Sharm Acl ReconstructionDocument7 pagesVivek Sharm Acl ReconstructionJuan Pablo FuentesNo ratings yet
- Peroneal Tendon InjuriesDocument12 pagesPeroneal Tendon InjuriesSamuel LauNo ratings yet
- Jurnal Shoulder Dislocation - PendekDocument84 pagesJurnal Shoulder Dislocation - PendekCliff LewisNo ratings yet
- Knee BiomechanicsDocument32 pagesKnee BiomechanicsnishantsinghbmeNo ratings yet
- Zones of Hand: Rose Mary AntonyDocument36 pagesZones of Hand: Rose Mary AntonyFatra FasyaNo ratings yet
- Below Knee and Through Knee ProsthesisDocument4 pagesBelow Knee and Through Knee ProsthesisClang TejadaNo ratings yet
- Radiography of The Hip: Lines, Signs, and Patterns of DiseaseDocument16 pagesRadiography of The Hip: Lines, Signs, and Patterns of DiseaseVivi Evita DewiNo ratings yet
- Lect 8 Lower Extremity Fracture 2Document22 pagesLect 8 Lower Extremity Fracture 220-221 Crisny Novika Yely Br. HutagaolNo ratings yet
- The Functional Anatomy of The Knee JointDocument12 pagesThe Functional Anatomy of The Knee JointFadzlee SoujiNo ratings yet
- Avascular Necrosis of The Fibular SesamoidDocument7 pagesAvascular Necrosis of The Fibular SesamoidAlex Yvan Escobedo HinostrozaNo ratings yet
- Soft Tissue Balance KneeDocument10 pagesSoft Tissue Balance KneeNitin BansalNo ratings yet
- Achilles Tendon RuptureDocument19 pagesAchilles Tendon Ruptureapi-509245925No ratings yet
- Arm:Leg Fracture PDFDocument11 pagesArm:Leg Fracture PDFHannaNo ratings yet
- Scolio SIS: Submitted ToDocument10 pagesScolio SIS: Submitted Tojean thereseNo ratings yet
- Ligamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDDocument35 pagesLigamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDAnonymous kdBDppigENo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- Ankle Fractures: A Literature Review of Current Treatment MethodsDocument13 pagesAnkle Fractures: A Literature Review of Current Treatment Methodsadrian1989No ratings yet
- KyphosisDocument32 pagesKyphosisBeniamin CostinașNo ratings yet
- Oh My Painful FOOT!!!: Plantar FasciitisDocument20 pagesOh My Painful FOOT!!!: Plantar FasciitisAsogaa MeteranNo ratings yet
- Anatomy of Spine: DR Pankaj N Surange MBBS, MD, Fipp Interventional Pain and Spine SpecialistDocument72 pagesAnatomy of Spine: DR Pankaj N Surange MBBS, MD, Fipp Interventional Pain and Spine SpecialistMohammad Riedho Cahya AtazsuNo ratings yet
- Thesis TopicDocument5 pagesThesis TopicSrikant KonchadaNo ratings yet
- ICF-Ankle Trimalleolar FractureDocument18 pagesICF-Ankle Trimalleolar FracturedvenumohanNo ratings yet
- ACL Injury PresentationDocument36 pagesACL Injury Presentationmail_rajibNo ratings yet
- Management of FractureDocument20 pagesManagement of FractureHitesh RohitNo ratings yet
- Adult Acquired Flatfoot DeformityDocument9 pagesAdult Acquired Flatfoot DeformityPutri ArthaNo ratings yet
- Ankle Fractures: Dr. T. VikramDocument35 pagesAnkle Fractures: Dr. T. VikramVicky VikramNo ratings yet
- Dance Injuries-Foot and AnkleDocument7 pagesDance Injuries-Foot and Ankleapi-198787605100% (1)
- Basic Principles of Tendon TransferDocument10 pagesBasic Principles of Tendon TransferyeapdshengNo ratings yet
- Flexor Tendon InjuriesDocument12 pagesFlexor Tendon InjuriesFrancis CarterNo ratings yet
- KAFODocument34 pagesKAFOBedo GikryNo ratings yet
- AO Trauma Vol.2Document100 pagesAO Trauma Vol.2Cujba GheorgheNo ratings yet
- Ankle Foot OrthosesDocument14 pagesAnkle Foot OrthosesNida MustafaNo ratings yet
- Biomechanics of KneeDocument48 pagesBiomechanics of KneeGavi Krishna100% (1)
- Flexor Tendon Injuries SeminarDocument75 pagesFlexor Tendon Injuries SeminarAmit GoyalNo ratings yet
- Lower Limb - Exam AnswersDocument27 pagesLower Limb - Exam AnswersAvi CNo ratings yet
- Ankle Instability: Dr. Syarif Hidayatullah, SP - OT, M.KesDocument75 pagesAnkle Instability: Dr. Syarif Hidayatullah, SP - OT, M.Kesahmad zakyNo ratings yet
- Acetabular and Hip FractureDocument133 pagesAcetabular and Hip FractureJuanita HenryNo ratings yet
- MCL Injury PaperDocument6 pagesMCL Injury Paperapi-268835137No ratings yet
- Chapter 11 NotesDocument12 pagesChapter 11 NotesAzwar Arsyad S SiNo ratings yet
- Total Hip Replacement PPDocument22 pagesTotal Hip Replacement PPAnonymous dGfXuDd5No ratings yet
- AmputationsDocument66 pagesAmputationsM Lateef GanaieNo ratings yet
- Any PDFDocument252 pagesAny PDFRaja VeerappanNo ratings yet
- Humeral Shaft FractureDocument82 pagesHumeral Shaft FractureYoga AninditaNo ratings yet
- Normal Human Posture: Anumol 2 Year Bpo Iipo ChennaiDocument25 pagesNormal Human Posture: Anumol 2 Year Bpo Iipo ChennaiIipo ChennaiNo ratings yet
- Orthosis For Sports InjuryDocument38 pagesOrthosis For Sports InjuryIipo ChennaiNo ratings yet
- Moment of InertiaDocument10 pagesMoment of InertiaIipo Chennai100% (1)
- CP SybpoDocument40 pagesCP SybpoIipo ChennaiNo ratings yet
- The Right of Persons With Disabilities To Live in The CommunityDocument35 pagesThe Right of Persons With Disabilities To Live in The CommunityIipo ChennaiNo ratings yet
- "The Problem Is Not How To Wipe - Rabindranath TagoreDocument43 pages"The Problem Is Not How To Wipe - Rabindranath TagoreIipo ChennaiNo ratings yet
- Review of Clinical Evidences in Orthotic Management of The Burn InjuriesDocument39 pagesReview of Clinical Evidences in Orthotic Management of The Burn InjuriesIipo ChennaiNo ratings yet
- Ifjp : Lafo/Kku Lhkk@La Kstu Ds Ekxz N"KZD Fu EDocument31 pagesIfjp : Lafo/Kku Lhkk@La Kstu Ds Ekxz N"KZD Fu EIipo ChennaiNo ratings yet
- CCRN Cert Review Neuro 2Document15 pagesCCRN Cert Review Neuro 2Giovanni MictilNo ratings yet
- Wernicke's EncephalopathyDocument39 pagesWernicke's Encephalopathyunbelievable686No ratings yet
- Thoracic Anesthesia Procedures Alan Kaye Ebook Full ChapterDocument51 pagesThoracic Anesthesia Procedures Alan Kaye Ebook Full Chapterholly.shelstad641100% (6)
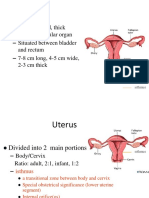
- SUPPORTS OF UTERUS ShilpaDocument61 pagesSUPPORTS OF UTERUS ShilpaSreelasya83% (6)
- Introduction To Physiology, Chemical Composition of The BodyDocument42 pagesIntroduction To Physiology, Chemical Composition of The Bodymrskhan jalalNo ratings yet
- 1 Living Things Living Thing: Secondary Biology Study Guide Aung Khant Kyaw Be (Ece), Delt (Eyu), Ma (English) 095127315Document28 pages1 Living Things Living Thing: Secondary Biology Study Guide Aung Khant Kyaw Be (Ece), Delt (Eyu), Ma (English) 095127315Aung Khant KyawNo ratings yet
- Code WDocument72 pagesCode Wmr warriorNo ratings yet
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- OT6 - Parkinson's DiseaseDocument5 pagesOT6 - Parkinson's DiseaseAnnbe BarteNo ratings yet
- Concept Map - Abby !Document2 pagesConcept Map - Abby !Abegail Abaygar100% (3)
- Tachycardia Approach and ManagementDocument41 pagesTachycardia Approach and ManagementChadi Alraies100% (5)
- Introduction To Anatomy Lecture 1: The Human Body: An OrientationDocument38 pagesIntroduction To Anatomy Lecture 1: The Human Body: An OrientationCupid MohNo ratings yet
- Radiol Clin N Am 2007 - Oral Cavity and Oropharynx TumorDocument20 pagesRadiol Clin N Am 2007 - Oral Cavity and Oropharynx Tumorgina2535No ratings yet
- Deadly Knife Targets 2011 PDFDocument1 pageDeadly Knife Targets 2011 PDFAnonymous B5pVvSXhNo ratings yet
- Livro - Acido LáticoDocument670 pagesLivro - Acido LáticoLuciana CoelhoNo ratings yet
- The Making of QiDocument11 pagesThe Making of Qiajardinera100% (1)
- Stress-Test - 3Document2 pagesStress-Test - 3api-491070484No ratings yet
- Week 01 - General AnatomyDocument17 pagesWeek 01 - General AnatomyTamene TekileNo ratings yet
- Patient Care MentoringDocument27 pagesPatient Care MentoringALrasshida TanNo ratings yet
- Fluids & ElectrolytesDocument18 pagesFluids & ElectrolytesBiway RegalaNo ratings yet
- Pathology of CNS TumorsDocument58 pagesPathology of CNS TumorsNaglaa RamadanNo ratings yet
- Astrand TestDocument33 pagesAstrand Testjayant rastogi100% (1)
- Subject Allocation Per Semestral Period: Brgy. Canarvacanan, Alcala, PangasinanDocument2 pagesSubject Allocation Per Semestral Period: Brgy. Canarvacanan, Alcala, PangasinanMike GuerzonNo ratings yet
- Neet PG 2012Document361 pagesNeet PG 2012Dhruvi PatelNo ratings yet
- Central Precocius PubertyDocument29 pagesCentral Precocius PubertyNurhidayat DayatNo ratings yet
- Soal Ujian Modul DasarDocument7 pagesSoal Ujian Modul DasarNikolas EdwinNo ratings yet
- 30day CH WorkBk - 2024 - HJDocument11 pages30day CH WorkBk - 2024 - HJShatabdi DashNo ratings yet
- Clas IficDocument9 pagesClas IficCristina GilcaNo ratings yet
- Kriya For Conquering SleepDocument4 pagesKriya For Conquering SleepKirpal JotyNo ratings yet
- Bromatology Paper PDFDocument8 pagesBromatology Paper PDFDrShivprasad MahadkarNo ratings yet