You might also like
- 847 - Protein Energy MalnutritionDocument20 pages847 - Protein Energy MalnutritionPriyanka Vikas TakNo ratings yet
- The Abnormal PuerperiumDocument25 pagesThe Abnormal PuerperiumMartijn JohanNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Week One: I. Origin of The Germ LineDocument67 pagesWeek One: I. Origin of The Germ LinerohitNo ratings yet
- Breast Self ExaminationDocument13 pagesBreast Self ExaminationChanDa DasNo ratings yet
- Wound Closure Methods: Sutures vs TapesDocument5 pagesWound Closure Methods: Sutures vs TapesINSANE LEO GAMINGNo ratings yet
- Spinal Cord InjuryDocument17 pagesSpinal Cord InjuryMuhammad FaridNo ratings yet
- PDF 075Document74 pagesPDF 075crystal_rc9No ratings yet
- TRAUMATIC PPH PREVENTION AND MANAGEMENTDocument30 pagesTRAUMATIC PPH PREVENTION AND MANAGEMENTRizwana BanuNo ratings yet
- Physiological Changes of The PuerperiumDocument6 pagesPhysiological Changes of The PuerperiumBladimir CentenoNo ratings yet
- Complications of Third Stage of Labour NishaDocument21 pagesComplications of Third Stage of Labour NishaSonia SapehiaNo ratings yet
- Causes and Types of Rapidly Progressive GlomerulonephritisDocument28 pagesCauses and Types of Rapidly Progressive GlomerulonephritisPaul SinsNo ratings yet
- Febrile Seizure Case FileDocument4 pagesFebrile Seizure Case Filehttps://medical-phd.blogspot.comNo ratings yet
- New Born Care: Catheter SuctioningDocument17 pagesNew Born Care: Catheter SuctioningRaffy100% (1)
- Benign Lesions of Vulva and VaginaDocument34 pagesBenign Lesions of Vulva and VaginaCabdiNo ratings yet
- Contraception: DR Husni SamarahDocument15 pagesContraception: DR Husni Samarahpal_pal_palNo ratings yet
- Rare Kidney Cancer in ChildrenDocument12 pagesRare Kidney Cancer in ChildrenKath CamachoNo ratings yet
- Tropical Splenomegaly SyndromeDocument12 pagesTropical Splenomegaly SyndromeSaidAandySaida100% (1)
- Gestational Age CalculationDocument7 pagesGestational Age CalculationDinesh Kumar100% (1)
- Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Document13 pagesCourse: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Leo D' GreatNo ratings yet
- ImmunotherapyDocument17 pagesImmunotherapyJonathan VenryNo ratings yet
- Operative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Document71 pagesOperative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Jhon Negesse100% (1)
- Trichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCDocument27 pagesTrichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCsushma shresthaNo ratings yet
- Hematology & Immune SystemDocument81 pagesHematology & Immune SystemAmanuel Maru100% (1)
- Bone Marrrow TransplantationDocument28 pagesBone Marrrow TransplantationvinoliNo ratings yet
- Puerperal PyrexiaDocument20 pagesPuerperal Pyrexiaهلا اكرم عقل طميزهNo ratings yet
- 63 Shock in Obstetrics & GynecologyDocument29 pages63 Shock in Obstetrics & GynecologyGodsonYeboah-AwudziNo ratings yet
- Pap Smear - Overview, Indications, PreparationDocument11 pagesPap Smear - Overview, Indications, PreparationBayu Surya DanaNo ratings yet
- HepatoblastomaDocument38 pagesHepatoblastomaSaroj PandaNo ratings yet
- FibroidDocument15 pagesFibroidNirupama KsNo ratings yet
- Genetic Screening and Prenatal DiagnosisDocument18 pagesGenetic Screening and Prenatal DiagnosisA B ONo ratings yet
- CTG Booklet: A Quick Reference Guide For Managing CtgsDocument16 pagesCTG Booklet: A Quick Reference Guide For Managing Ctgscirlce:twoworldsconnectedNo ratings yet
- The Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodDocument26 pagesThe Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodNabard MhammadNo ratings yet
- CAH Diagnosis and TreatmentDocument10 pagesCAH Diagnosis and TreatmentJemmy Wijaya100% (1)
- 050 PPT - RetinoblastomaDocument61 pages050 PPT - RetinoblastomaAnastasia TjanNo ratings yet
- Bullous Pemphigoid PosterDocument21 pagesBullous Pemphigoid PosterChe Ainil ZainodinNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad PrasadNo ratings yet
- Nephrotic SyndromeeDocument28 pagesNephrotic SyndromeeRiteka SinghNo ratings yet
- Chapter 14 - HematopathologyDocument66 pagesChapter 14 - Hematopathologynigel farageNo ratings yet
- Neonatal InfectionsDocument19 pagesNeonatal InfectionsA B Siddique RiponNo ratings yet
- Meningitis Seminar 1Document38 pagesMeningitis Seminar 1vani reddyNo ratings yet
- Essential facts about anemia in pregnancyDocument40 pagesEssential facts about anemia in pregnancyraph faith100% (1)
- Disseminated Intravascular CoagulationDocument4 pagesDisseminated Intravascular CoagulationHendra SshNo ratings yet
- PMTCTDocument26 pagesPMTCTMaxwell C Jay KafwaniNo ratings yet
- Contraceptive MethodsDocument40 pagesContraceptive MethodsMa. Lourdes CarbonillaNo ratings yet
- Identification of Microorganisms: Unknown SpecimensDocument10 pagesIdentification of Microorganisms: Unknown SpecimensAnonymous wVgEAr6No ratings yet
- Opthalmia UmDocument23 pagesOpthalmia Umnanu-jenuNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadNo ratings yet
- Notes On MicrotomeDocument10 pagesNotes On MicrotomeAnonymous HXLczq3No ratings yet
- Chapter 12 Conception and Fetal DevelopmentDocument17 pagesChapter 12 Conception and Fetal DevelopmentRoneshia Michelle Rudolph100% (1)
- Leukemia PDFDocument63 pagesLeukemia PDFErfan Syahid AzhariNo ratings yet
- Female Genital TuberculosisDocument6 pagesFemale Genital TuberculosisallauddinbarackzaiNo ratings yet
- Hemorrhagic Disease of The NewbornDocument2 pagesHemorrhagic Disease of The NewbornsucirahmiiiiiiNo ratings yet
- CryosurgeryDocument4 pagesCryosurgeryShaan SonuNo ratings yet
- Shaafi Medical College Obstetrics GuideDocument39 pagesShaafi Medical College Obstetrics Guidemustafe omarNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShaliniNo ratings yet
- Vacuum DeliveryDocument31 pagesVacuum DeliveryAparna LaxmanNo ratings yet
- Placenta and Fetal Membrane-6614Document45 pagesPlacenta and Fetal Membrane-6614Incredible DivineNo ratings yet
- Polyneuropathies and Conditions Like GBS and CIDPDocument26 pagesPolyneuropathies and Conditions Like GBS and CIDPCHANGEZ KHAN SARDARNo ratings yet
- Cricopharyngeal Myotomy Surgical TechniqueDocument8 pagesCricopharyngeal Myotomy Surgical TechniqueDANDYNo ratings yet
- Assessment and Management of Endo-Periodontal Lesions: DentistryDocument12 pagesAssessment and Management of Endo-Periodontal Lesions: Dentistryedgar curayNo ratings yet
- Maternal Midterm Reviewer Common ProblemsDocument58 pagesMaternal Midterm Reviewer Common ProblemsEya BaldostamonNo ratings yet
- Pregnancy Induced Hypertension Case StudyDocument54 pagesPregnancy Induced Hypertension Case Studysupernurse02No ratings yet
- Handbook of Drugs in Intensive Care GuideDocument6 pagesHandbook of Drugs in Intensive Care GuideardriangollerNo ratings yet
- Dermatology Study Guide 2021Document5 pagesDermatology Study Guide 2021Osmo SisNo ratings yet
- Radiology: Tadio Physics & Nuclear MedicimDocument33 pagesRadiology: Tadio Physics & Nuclear Medicimsk100% (1)
- AGA-DDSEP-10-Chapter-7-1653072629120 2Document34 pagesAGA-DDSEP-10-Chapter-7-1653072629120 2yyr4cdwcjdNo ratings yet
- Case Presentation On Pregnancy Induced Hypertension: Central Philippine University College of NursingDocument26 pagesCase Presentation On Pregnancy Induced Hypertension: Central Philippine University College of NursingromyNo ratings yet
- Nervous System Infections GuideDocument91 pagesNervous System Infections GuideBea Bianca CruzNo ratings yet
- MIB - Internal Medicine 2 Semester 8 Updated March 2021Document26 pagesMIB - Internal Medicine 2 Semester 8 Updated March 2021Kavin VarmaNo ratings yet
- Diseases of Nervous System of Farm Animals by Ali SadiekDocument65 pagesDiseases of Nervous System of Farm Animals by Ali SadiekAli H. Sadiek أ.د. علي حسن صديق100% (7)
- Cast in Urine SedimentDocument3 pagesCast in Urine Sedimentfirie100% (1)
- Peptic Ulcer DiseaseDocument4 pagesPeptic Ulcer DiseaseWidyan Muchzadi AkbarNo ratings yet
- Surgery OSCE Stations With KeyDocument274 pagesSurgery OSCE Stations With KeyMoazzam AliNo ratings yet
- Lecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Document58 pagesLecture & Review Guide in HEMATOLOGY 1 & 2 (COMPLETE)Kirt Anonuevo100% (3)
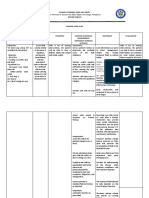
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument2 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKarl Lourenz DeysolongNo ratings yet
- Basic Neuroscience CompiledDocument71 pagesBasic Neuroscience CompiledDr.Rathod RanjithNo ratings yet
- Facial Pain, Headache, and Otalgia: Khristine T. Girado - Pizarro, MD, FPSO-HNSDocument18 pagesFacial Pain, Headache, and Otalgia: Khristine T. Girado - Pizarro, MD, FPSO-HNSAria Jean MostajoNo ratings yet
- Intussusception: Dr. Narendra Singh Shekhawat Assistant Professor Department of Shalya TantraDocument21 pagesIntussusception: Dr. Narendra Singh Shekhawat Assistant Professor Department of Shalya TantrakhushbuNo ratings yet
- Grading Sheet SPADocument1 pageGrading Sheet SPAMike BoribsNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Inflammatory Bowel Disease: Professor Ravi KantDocument24 pagesInflammatory Bowel Disease: Professor Ravi KantIndah MutiaraNo ratings yet
- Rina Ramayani Komplikasi SN KONIKA XVIIDocument26 pagesRina Ramayani Komplikasi SN KONIKA XVIIirene aureliaNo ratings yet
- Carbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistryDocument93 pagesCarbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistrySimham Venu0% (1)
- BP6 15depression PDFDocument75 pagesBP6 15depression PDFada ramosNo ratings yet
- Surgical Pathology of Liver TumorsDocument480 pagesSurgical Pathology of Liver TumorsGeorgiana BuhociNo ratings yet
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case Study19lyon92100% (6)
- Research Publications in Ayurvedic SciencesDocument1,231 pagesResearch Publications in Ayurvedic SciencesYuvraj HanwateNo ratings yet