You might also like
- CHLAMYDIADocument9 pagesCHLAMYDIAFatima AbasovaNo ratings yet
- Mycoplasma Pneumonia DiscussionDocument18 pagesMycoplasma Pneumonia Discussionmuskaanmir108No ratings yet
- 1.8 The ChlamydiaDocument21 pages1.8 The ChlamydiaNkululeko SinethembaNo ratings yet
- Chlamydia by Rosemary C. AgboDocument24 pagesChlamydia by Rosemary C. AgboRosemaryNo ratings yet
- Ophthalmia NeonatorumDocument2 pagesOphthalmia NeonatorumjudssalangsangNo ratings yet
- ChlamydiaDocument3 pagesChlamydiaMZ LimNo ratings yet
- Caso Clínico - Neisseria GonorrhoeaeDocument7 pagesCaso Clínico - Neisseria GonorrhoeaeRigobertoNo ratings yet
- Pneumococcus PneumoniaDocument20 pagesPneumococcus PneumoniaIseoghenaNo ratings yet
- Caso Clínico - Chlamydia TrachomatisDocument4 pagesCaso Clínico - Chlamydia TrachomatisRigobertoNo ratings yet
- MICROPARA!Document5 pagesMICROPARA!mememe22No ratings yet
- Lecture Rickettsia Chlamydia, MycoplasmaDocument49 pagesLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- Solis PT WK 8Document3 pagesSolis PT WK 8Niña ReyesNo ratings yet
- MICROBIOLOGY Pathogenic Gram-Positive Bacilli (Corynebacterium)Document7 pagesMICROBIOLOGY Pathogenic Gram-Positive Bacilli (Corynebacterium)Ravindra SinghNo ratings yet
- Pathophysiology of Tuberculosis: Pratik Godhani Pharmacy ManagementDocument15 pagesPathophysiology of Tuberculosis: Pratik Godhani Pharmacy ManagementPratik GodhaniNo ratings yet
- PneumoniaDocument10 pagesPneumoniaAubrey PerezNo ratings yet
- RespiratoryDocument57 pagesRespiratoryMuhammad Javed GabaNo ratings yet
- Pneumonia Caused by Chlamydia Pneumoniae in ChildrenDocument19 pagesPneumonia Caused by Chlamydia Pneumoniae in Childrenmayteveronica1000No ratings yet
- Sexual Transmitted InfectionsDocument44 pagesSexual Transmitted InfectionsDeshielanny AlagumolyNo ratings yet
- Measles: EtiologyDocument14 pagesMeasles: EtiologyHan SANo ratings yet
- Bakteri Penyebab IMSDocument67 pagesBakteri Penyebab IMSuut14No ratings yet
- Neisseria & Moraxella: Done By: Tamara Khalel, Majd Shweiki, Aya SulimanDocument22 pagesNeisseria & Moraxella: Done By: Tamara Khalel, Majd Shweiki, Aya SulimanSalih TahsinNo ratings yet
- Klebsiella Pneumoniae Pathogenesis: Etiology/BacteriologyDocument4 pagesKlebsiella Pneumoniae Pathogenesis: Etiology/Bacteriologysuper cute100% (1)
- Pleuropulmonary InfectionsDocument40 pagesPleuropulmonary InfectionsRahmidatul AftikaNo ratings yet
- M Pneumoniae,: Community-Acquired PneumoniaDocument3 pagesM Pneumoniae,: Community-Acquired PneumoniaOlaru CatalinaNo ratings yet
- ChlamydiaDocument22 pagesChlamydiadelia rahmaNo ratings yet
- Infections of The Central Nervous System: DR John Egbagba FmcpathDocument46 pagesInfections of The Central Nervous System: DR John Egbagba FmcpathPrincewill SeiyefaNo ratings yet
- Ophthalmia NeonatorumDocument2 pagesOphthalmia NeonatorumEjay BautistaNo ratings yet
- ChlamydiaDocument13 pagesChlamydiaTitus MutwiriNo ratings yet
- Syphilis: Michelle LinardiDocument20 pagesSyphilis: Michelle Linardimichelle95No ratings yet
- Chapter 13Document8 pagesChapter 13Marah MazahrehNo ratings yet
- Crypto Cocco SisDocument32 pagesCrypto Cocco SisLincy JohnyNo ratings yet
- Severe Acute Cytomegalovirus Sialadenitis in An Immunocompetent Adult: Case ReportDocument2 pagesSevere Acute Cytomegalovirus Sialadenitis in An Immunocompetent Adult: Case ReportanimegawatiNo ratings yet
- Cap 25 AprilDocument57 pagesCap 25 AprilAnuNo ratings yet
- ConjunctivitisDocument113 pagesConjunctivitisHussam AliNo ratings yet
- New Chapter 3 Medical Microbiology (1) 2Document130 pagesNew Chapter 3 Medical Microbiology (1) 2Rani Faed SabraNo ratings yet
- Ophthalmia neonatorumIIDocument29 pagesOphthalmia neonatorumIIgopscharanNo ratings yet
- Lecture 13 - Medical Mycology - HistoplasmosisDocument18 pagesLecture 13 - Medical Mycology - Histoplasmosissinghak203akNo ratings yet
- Neisseria Meningitidis: General ConceptsDocument16 pagesNeisseria Meningitidis: General Conceptssomebody_maNo ratings yet
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini60% (5)
- Page Two 100509ToxoplasmaGondiinfectsMostSpeciesPage2Document2 pagesPage Two 100509ToxoplasmaGondiinfectsMostSpeciesPage2Ralph Charles Whitley, Sr.No ratings yet
- Pelvic Infections in Women: Belgian Guidelines: OutlineDocument35 pagesPelvic Infections in Women: Belgian Guidelines: OutlineJose mauricio PalenciaNo ratings yet
- Micro ChAP 15Document34 pagesMicro ChAP 15Farah ZahidNo ratings yet
- (KATING) Haemophilus DucreyiDocument16 pages(KATING) Haemophilus DucreyiIda Bagus Putu SwabawaNo ratings yet
- Case Study 1: Group 1Document27 pagesCase Study 1: Group 1Jennylen TorresNo ratings yet
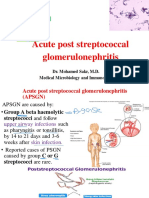
- Micro PSGNDocument32 pagesMicro PSGNMahmoud hilmyNo ratings yet
- Opthalmia UmDocument23 pagesOpthalmia Umnanu-jenuNo ratings yet
- 2017 Sept ReviewDocument7 pages2017 Sept ReviewJem QuintoNo ratings yet
- Document 3Document3 pagesDocument 3theresia 102018040No ratings yet
- MycoplasmaDocument2 pagesMycoplasmaHisham ChomanyNo ratings yet
- Ophthalmia NeonatorumDocument30 pagesOphthalmia NeonatorumLing TaerahkunNo ratings yet
- Pneumonia With Pleural EffusionDocument24 pagesPneumonia With Pleural EffusionMund CheleNo ratings yet
- Sexually Transmmited Diseases: Presenter: Nyangara Rajabu Facilitator: Isaac U. MDocument31 pagesSexually Transmmited Diseases: Presenter: Nyangara Rajabu Facilitator: Isaac U. MnyangaraNo ratings yet
- 2 Gram Negative Bacterial InfectionDocument89 pages2 Gram Negative Bacterial InfectionCoy NuñezNo ratings yet
- Final Case Study of Cap EditDocument50 pagesFinal Case Study of Cap EditBem Bem Kai Hinoguin100% (1)
- Other Bacteria With Unusual Growth Requirements PDFDocument102 pagesOther Bacteria With Unusual Growth Requirements PDFNova Amor MahayagNo ratings yet
- NeisseriaDocument32 pagesNeisseriaKeshant SamarooNo ratings yet
- Haemophilus DucreyiDocument15 pagesHaemophilus DucreyichristieNo ratings yet
- Oral Cancer Lesson PlanDocument10 pagesOral Cancer Lesson Planapi-543973374100% (1)
- Endocrine MedicationsDocument47 pagesEndocrine MedicationsAamir AzizNo ratings yet
- Maternal and ChildDocument45 pagesMaternal and ChildShiela Joy DuquezNo ratings yet
- Cultural Competency For Recovery Coache1Document22 pagesCultural Competency For Recovery Coache1IlannaSharonMandelNo ratings yet
- Candidiasis: Armie Jade S. Gante, RNDocument18 pagesCandidiasis: Armie Jade S. Gante, RNAnnapurna DangetiNo ratings yet
- Sop CFLTC 14.06.20Document55 pagesSop CFLTC 14.06.20madhusoodhananppNo ratings yet
- Heterogeneity in Statistical Genetics: Derek Gordon Stephen J. Finch Wonkuk KimDocument366 pagesHeterogeneity in Statistical Genetics: Derek Gordon Stephen J. Finch Wonkuk KimWulil AlbabNo ratings yet
- Quarters 1 and 2 - Module 8: Optimizing Your Health Through Physical ActivitiesDocument22 pagesQuarters 1 and 2 - Module 8: Optimizing Your Health Through Physical ActivitiesRussel MejicoNo ratings yet
- UMP Assingement (PRINCIPLES OF SAFETY ENGINEERING)Document15 pagesUMP Assingement (PRINCIPLES OF SAFETY ENGINEERING)Yogendran SundrasaigramNo ratings yet
- Adverse Drug ReactionDocument7 pagesAdverse Drug ReactionufahadNo ratings yet
- Dr. Zaka Ur Rab Siddiqui - Senior Surgeon Laparoscopic-Bariatric Frcs-Fcps-MrcsDocument5 pagesDr. Zaka Ur Rab Siddiqui - Senior Surgeon Laparoscopic-Bariatric Frcs-Fcps-MrcscdeekyNo ratings yet
- FON Mcqs..-1Document2 pagesFON Mcqs..-1Rizwan EjazNo ratings yet
- Dystonia and Its Treatment in Ehlers Danlos SyndromeDocument5 pagesDystonia and Its Treatment in Ehlers Danlos Syndromeannie baiNo ratings yet
- Battered Child Syndrome (BCS) : Physical SignsDocument4 pagesBattered Child Syndrome (BCS) : Physical SignssabinNo ratings yet
- Endocrine and Metabolic DisordersDocument64 pagesEndocrine and Metabolic DisordersSyahrul Tuba Al FatihNo ratings yet
- King, Albert I - The Biomechanics of Impact Injury - Biomechanical Response, Mechanisms of Injury, Human Tolerance and SimulationDocument706 pagesKing, Albert I - The Biomechanics of Impact Injury - Biomechanical Response, Mechanisms of Injury, Human Tolerance and SimulationLuis7929100% (1)
- Ascites Case PresentationDocument44 pagesAscites Case PresentationAman Mehla75% (4)
- 001 - 976 - Ratih Purnamasari Nukana - GalleyDocument6 pages001 - 976 - Ratih Purnamasari Nukana - GalleyWenasNo ratings yet
- Vascular Diseases For The Non-SpecialistDocument279 pagesVascular Diseases For The Non-SpecialistHîrjoabă Ioan100% (1)
- Probiotics and Prebiotics: International Journal of Current Research December 2018Document13 pagesProbiotics and Prebiotics: International Journal of Current Research December 2018Maï SsaNo ratings yet
- MCN MT 1Document23 pagesMCN MT 1Jekka Ann Dela CruzNo ratings yet
- Dr. Sebi Fast and Kidney Flush IngredientsDocument8 pagesDr. Sebi Fast and Kidney Flush IngredientsSoror OnyxNo ratings yet
- Infrastructure Law Project FinalDocument22 pagesInfrastructure Law Project FinalHarshit MalviyaNo ratings yet
- Management of Lower Extremity TraumaDocument34 pagesManagement of Lower Extremity Trauma정형화No ratings yet
- June-2020 Public-Health-BulletinDocument2 pagesJune-2020 Public-Health-Bulletinapi-520055210No ratings yet
- Gastroesophageal Reflux DiseaseDocument8 pagesGastroesophageal Reflux DiseaseGOURINANDHANo ratings yet
- Long Term Effects of Child Abuse Draft 2 2Document11 pagesLong Term Effects of Child Abuse Draft 2 2api-548856677No ratings yet
- Schizotypal Personality Disorder by SlidesgoDocument40 pagesSchizotypal Personality Disorder by SlidesgoLismery ReyesNo ratings yet
- Prefix-Meanings: Kisen Kaisha D. Bautista, MDDocument4 pagesPrefix-Meanings: Kisen Kaisha D. Bautista, MDKisen DiazNo ratings yet
- Testing For COVID-19Document2 pagesTesting For COVID-19oanaNo ratings yet