You might also like
- Laboratory Diagnosis of CancerDocument47 pagesLaboratory Diagnosis of Cancerdr_asr100% (8)
- 1 Raven's™ Standard Progressive Matrices Plus (SPM Plus) - PSI OnlineDocument1 page1 Raven's™ Standard Progressive Matrices Plus (SPM Plus) - PSI OnlineVINEET GAIROLANo ratings yet
- Alopez Craiva 16 WHO UpdateDocument87 pagesAlopez Craiva 16 WHO UpdateDima PathNo ratings yet
- Undifferentiated Panel: Ca Vs Mel Vs LaDocument12 pagesUndifferentiated Panel: Ca Vs Mel Vs LaAndres RestrepoNo ratings yet
- Immunohistochemical MarkersDocument12 pagesImmunohistochemical MarkersAsmara SyedNo ratings yet
- Singapore SalivaryDocument149 pagesSingapore Salivaryna huNo ratings yet
- Update in Salivary Gland Pathology: Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016Document68 pagesUpdate in Salivary Gland Pathology: Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016gugicevdzoceNo ratings yet
- Next Gen IHC For Soft Tissue Diagnosis Hornick 7 Jan 2023Document74 pagesNext Gen IHC For Soft Tissue Diagnosis Hornick 7 Jan 2023na huNo ratings yet
- Urogenital TumorDocument71 pagesUrogenital TumorJanet UngNo ratings yet
- Multiple Myeloma FinalDocument69 pagesMultiple Myeloma FinalMoinuddin_ReffaiNo ratings yet
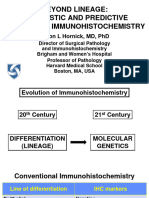
- Hornick Beyond Lineage 8 June 1035Document96 pagesHornick Beyond Lineage 8 June 1035Olteanu Dragos-NicolaeNo ratings yet
- AML Pita DR MardiahDocument71 pagesAML Pita DR MardiahSarly Puspita AriesaNo ratings yet
- Multiple Myeloma: LT Col Vivek AggarwalDocument42 pagesMultiple Myeloma: LT Col Vivek AggarwalShravan Rakaraddi100% (2)
- Multiple MyelomaDocument23 pagesMultiple Myelomabubbu92No ratings yet
- NEOPLASIADocument15 pagesNEOPLASIADr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Hornick Carcinoma of Unknown Primary 8 June 1400Document87 pagesHornick Carcinoma of Unknown Primary 8 June 1400Olteanu Dragos-NicolaeNo ratings yet
- Multiple Myeloma: Presented By: DR - Ramesh Kumar Guide:-Dr. O.P. Meena SirDocument65 pagesMultiple Myeloma: Presented By: DR - Ramesh Kumar Guide:-Dr. O.P. Meena Sirvikash meenaNo ratings yet
- CH 34 / CH 76 Neoplasms of The Testis: 11th 12thDocument77 pagesCH 34 / CH 76 Neoplasms of The Testis: 11th 12thSirawit Namkaeng ChoksuchatNo ratings yet
- Rimmer SPEP Multiple MyelomaDocument35 pagesRimmer SPEP Multiple MyelomaAaron AntonioNo ratings yet
- Multiple Myeloma A New Treatment ApproachDocument27 pagesMultiple Myeloma A New Treatment ApproachIndonesian Journal of Cancer100% (1)
- 25 Yo Male With Fever of 1month Duration HB 5.0gm/dl TLC: 70,000 Cells/cumm Platelets: 40,000/cummDocument47 pages25 Yo Male With Fever of 1month Duration HB 5.0gm/dl TLC: 70,000 Cells/cumm Platelets: 40,000/cummMahalakshmi PalanisamiNo ratings yet
- Biologyandpathophysiologyofcancer 13178331101958 Phpapp01 111005115351 Phpapp01Document87 pagesBiologyandpathophysiologyofcancer 13178331101958 Phpapp01 111005115351 Phpapp01pusatdatagizi soewondokendalNo ratings yet
- Epk FDocument73 pagesEpk FBryan FjbNo ratings yet
- ALopezBeltran Craiova 16 Patron InvertidoDocument54 pagesALopezBeltran Craiova 16 Patron InvertidoDima PathNo ratings yet
- Acute Myeloid LeukemiaDocument29 pagesAcute Myeloid LeukemiaMohammad Fadel Satriansyah100% (1)
- Colorectal Polyps and Adenoma-Carcinoma SequenceDocument26 pagesColorectal Polyps and Adenoma-Carcinoma SequenceSonnitorontoNo ratings yet
- Plasma Cell NeoplasmsDocument36 pagesPlasma Cell Neoplasmsdrafq2000No ratings yet
- Unknown Primary - Diagnostic Approach Using IHC Hornick 7 Jan 2023Document70 pagesUnknown Primary - Diagnostic Approach Using IHC Hornick 7 Jan 2023na huNo ratings yet
- Tumor Markers: Michael A. Pesce, PHD Department of Pathology Columbia-Presbyterian Medical CenterDocument28 pagesTumor Markers: Michael A. Pesce, PHD Department of Pathology Columbia-Presbyterian Medical CenterGopalrao VallepuNo ratings yet
- Salivaryglandtumors 150912063235 Lva1 App6892Document213 pagesSalivaryglandtumors 150912063235 Lva1 App6892Waqas IqbalNo ratings yet
- Slide Microteaching MM Iqbal 2Document40 pagesSlide Microteaching MM Iqbal 2RAJA HARAHAPNo ratings yet
- Monoclonal GammopathiesDocument70 pagesMonoclonal GammopathiesElisa Lincă100% (1)
- Acute Myeloid Leukemia - AML: Clinical BackgroundDocument12 pagesAcute Myeloid Leukemia - AML: Clinical BackgroundNyxa AbdullaNo ratings yet
- Lung Carcinomas New 2015 WHO Classification Histopathology of NSCLC, IHC Markers and WHO ClassificationDocument34 pagesLung Carcinomas New 2015 WHO Classification Histopathology of NSCLC, IHC Markers and WHO ClassificationAna Maria Torres LopezNo ratings yet
- Dr. Asifa Iqbal Oral and Maxillofacial Surgery, KEMU Mayo Hospital, LahoreDocument53 pagesDr. Asifa Iqbal Oral and Maxillofacial Surgery, KEMU Mayo Hospital, LahoreAl RawdhaNo ratings yet
- Leucemias Agudas: Kenny Mauricio Galvez HematologiaDocument62 pagesLeucemias Agudas: Kenny Mauricio Galvez HematologiaMichelle Ocampo ValenciaNo ratings yet
- Childhood CancerDocument16 pagesChildhood CancerNovia Khoerunnisa100% (2)
- STT 2Document57 pagesSTT 2Safrilia GandhiNo ratings yet
- Kolorektal & Anus: Dr. Yusmaidi, SP.BDocument104 pagesKolorektal & Anus: Dr. Yusmaidi, SP.BAsmorowatiNo ratings yet
- Patho - 4th Assessment - Plasma Cell Neoplasms - 28 Jan 2007Document28 pagesPatho - 4th Assessment - Plasma Cell Neoplasms - 28 Jan 2007api-3703352No ratings yet
- Session 8 Visser Haematology Topo MorphoDocument34 pagesSession 8 Visser Haematology Topo MorphoMaradonaNo ratings yet
- Tumor Urogenital: Dr. Hariyono, SpuDocument42 pagesTumor Urogenital: Dr. Hariyono, SpumelianyNo ratings yet
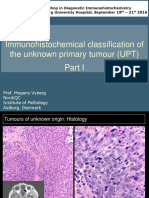
- Immunohistochemical Classification of The Unknown Primary Tumour (UPT)Document87 pagesImmunohistochemical Classification of The Unknown Primary Tumour (UPT)Abhugz VosotrosNo ratings yet
- ThyroidDocument102 pagesThyroidfadoNo ratings yet
- Salivary Glands TumoursDocument102 pagesSalivary Glands TumoursSokna SyNo ratings yet
- Myeloproliferative Disorders / Neoplasms Intro For The InternistDocument37 pagesMyeloproliferative Disorders / Neoplasms Intro For The InternistrodtobingNo ratings yet
- Carcinoma InsituDocument46 pagesCarcinoma InsituminnalesriNo ratings yet
- Tumor IntraabdomenDocument30 pagesTumor IntraabdomenBedahanakugmNo ratings yet
- Myeloproliferative Disorders / Neoplasms Intro For The InternistDocument37 pagesMyeloproliferative Disorders / Neoplasms Intro For The InternistityNo ratings yet
- Small Cell Lung Cancer (SCLC) and Tkis in NSCLCDocument73 pagesSmall Cell Lung Cancer (SCLC) and Tkis in NSCLCAgi Azhari SandiniNo ratings yet
- UrooncologyDocument49 pagesUrooncologyanwar jabariNo ratings yet
- Testicular TumorDocument71 pagesTesticular TumorJohannes MarpaungNo ratings yet
- GENITOURINARY CANCER 1 Final Euyyy (Recovered)Document36 pagesGENITOURINARY CANCER 1 Final Euyyy (Recovered)Harry FaisalNo ratings yet
- MMDocument67 pagesMMRatnaNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Molecular Basis of Cancer: Nethravathi R GN113011Document51 pagesMolecular Basis of Cancer: Nethravathi R GN113011manuel1788No ratings yet
- Clinical GuidlinesDocument200 pagesClinical GuidlinesMujtaba NadeemNo ratings yet
- Current Diagnosis and Classification of Hematological MalignanciesDocument59 pagesCurrent Diagnosis and Classification of Hematological Malignanciesedel_herbityaNo ratings yet
- Tumour GeneticsDocument43 pagesTumour Geneticsmalaz197No ratings yet
- Genitourinary Tract Tumors Including Renal Tumors: Pre-ReadingDocument31 pagesGenitourinary Tract Tumors Including Renal Tumors: Pre-Readingmus zaharaNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Nipple Discharge 3Document3 pagesNipple Discharge 3Dima PathNo ratings yet
- Acino in BreastDocument2 pagesAcino in BreastDima PathNo ratings yet
- ST Gallen 2011Document6 pagesST Gallen 2011Dima PathNo ratings yet
- Tamoxifen in Breast CADocument14 pagesTamoxifen in Breast CADima PathNo ratings yet
- Podopl in Breast CA Mod Pathol2012Document15 pagesPodopl in Breast CA Mod Pathol2012Dima PathNo ratings yet
- ACC Breast JapDocument4 pagesACC Breast JapDima PathNo ratings yet
- ACC Is Not Secretory CaDocument7 pagesACC Is Not Secretory CaDima PathNo ratings yet
- SN ITC SignificatoDocument10 pagesSN ITC SignificatoDima PathNo ratings yet
- Acta Cytol2010Document3 pagesActa Cytol2010Dima PathNo ratings yet
- FAN-CB Breast 2012Document7 pagesFAN-CB Breast 2012Dima PathNo ratings yet
- ALopezBeltran Craiova 16 Patron InvertidoDocument54 pagesALopezBeltran Craiova 16 Patron InvertidoDima PathNo ratings yet
- FNAC Axillary 2012Document9 pagesFNAC Axillary 2012Dima PathNo ratings yet
- ACC BreastDocument4 pagesACC BreastDima PathNo ratings yet
- Pathologi Complete Response To TherapyDocument5 pagesPathologi Complete Response To TherapyDima PathNo ratings yet
- FNAC Male Breast RevDocument6 pagesFNAC Male Breast RevDima PathNo ratings yet
- FNAC Male BreastDocument5 pagesFNAC Male BreastDima PathNo ratings yet
- FNAC AuditDocument6 pagesFNAC AuditDima PathNo ratings yet
- FNAC Axillary 2012bDocument7 pagesFNAC Axillary 2012bDima PathNo ratings yet
- Sick Lobe 12 GöteborgDocument140 pagesSick Lobe 12 GöteborgDima PathNo ratings yet
- Sick Lobe ST 2008Document109 pagesSick Lobe ST 2008Dima PathNo ratings yet
- Alopez Craiva 16 Variants Invasive Bladd CancerDocument115 pagesAlopez Craiva 16 Variants Invasive Bladd CancerDima PathNo ratings yet
- Ihc ColecchiaDocument32 pagesIhc ColecchiaDima PathNo ratings yet
- Iccr PenisDocument19 pagesIccr PenisDima PathNo ratings yet
- Who Update PenisDocument38 pagesWho Update PenisDima PathNo ratings yet
- Colecchia Who Non Germ Cell Tumors UpdateDocument65 pagesColecchia Who Non Germ Cell Tumors UpdateDima PathNo ratings yet
- Frozen Section DiagnosisDocument290 pagesFrozen Section DiagnosisDima PathNo ratings yet
- BLDG Permit Form (Back To Back)Document2 pagesBLDG Permit Form (Back To Back)ar desNo ratings yet
- Pro Con ChartDocument3 pagesPro Con Chartapi-461614875No ratings yet
- Theories of GrowthDocument33 pagesTheories of Growthdr parveen bathlaNo ratings yet
- Tasha Giles: WebsiteDocument1 pageTasha Giles: Websiteapi-395325861No ratings yet
- Emerging and Less Common Viral Encephalitides - Chapter 91Document34 pagesEmerging and Less Common Viral Encephalitides - Chapter 91Victro ChongNo ratings yet
- Reading Comprehension Lesson Plan FinalDocument9 pagesReading Comprehension Lesson Plan Finalapi-254917183No ratings yet
- Class XI-Writing-Job ApplicationDocument13 pagesClass XI-Writing-Job Applicationisnprincipal2020No ratings yet
- Manual Safety Installation Operations Tescom en 123946Document23 pagesManual Safety Installation Operations Tescom en 123946Karikalan JayNo ratings yet
- Light Design by Anil ValiaDocument10 pagesLight Design by Anil ValiaMili Jain0% (1)
- File Server Resource ManagerDocument9 pagesFile Server Resource ManagerBùi Đình NhuNo ratings yet
- Development and Application of "Green," Environmentally Friendly Refractory Materials For The High-Temperature Technologies in Iron and Steel ProductionDocument6 pagesDevelopment and Application of "Green," Environmentally Friendly Refractory Materials For The High-Temperature Technologies in Iron and Steel ProductionJJNo ratings yet
- FinancialAccountingTally PDFDocument1 pageFinancialAccountingTally PDFGurjot Singh RihalNo ratings yet
- Gregorian-Lunar Calendar Conversion Table of 1960 (Geng-Zi - Year of The Mouse)Document1 pageGregorian-Lunar Calendar Conversion Table of 1960 (Geng-Zi - Year of The Mouse)Anomali SahamNo ratings yet
- A. Erfurth, P. Hoff. Mad Scenes in Early 19th-Century Opera PDFDocument4 pagesA. Erfurth, P. Hoff. Mad Scenes in Early 19th-Century Opera PDFbiarrodNo ratings yet
- Test Bank For Macroeconomics 8th Canadian Edition Andrew AbelDocument16 pagesTest Bank For Macroeconomics 8th Canadian Edition Andrew AbelstebinrothNo ratings yet
- AMST 398 SyllabusDocument7 pagesAMST 398 SyllabusNatNo ratings yet
- Removal of Chloride in The Kraft Chemical Recovery CycleDocument8 pagesRemoval of Chloride in The Kraft Chemical Recovery CycleVeldaa AmiraaNo ratings yet
- Part-II Poem Article and Report For College Magazine-2015-16 Dr.M.Q. KhanDocument4 pagesPart-II Poem Article and Report For College Magazine-2015-16 Dr.M.Q. KhanTechi Son taraNo ratings yet
- Ap Reg W# 5-Scaffold For Transfer TemplateDocument2 pagesAp Reg W# 5-Scaffold For Transfer TemplateJunafel Boiser Garcia100% (2)
- Introduction To Hydraulic System in The Construction Machinery - Copy ALIDocument2 pagesIntroduction To Hydraulic System in The Construction Machinery - Copy ALImahadNo ratings yet
- Extension of MDRRMO OfficeDocument12 pagesExtension of MDRRMO OfficeJustin YuabNo ratings yet
- ICCM2014Document28 pagesICCM2014chenlei07No ratings yet
- University Physics With Modern Physics 2nd Edition Bauer Test BankDocument24 pagesUniversity Physics With Modern Physics 2nd Edition Bauer Test BankJustinTaylorepga100% (42)
- A3 Report Template Checklist - SafetyCultureDocument4 pagesA3 Report Template Checklist - SafetyCulturewarriorninNo ratings yet
- 08 - Chapter 1Document48 pages08 - Chapter 1danfm97No ratings yet
- Edwards SVV HandoutDocument2 pagesEdwards SVV HandoutossinNo ratings yet
- MHD Exam 6 MaterialDocument179 pagesMHD Exam 6 Materialnaexuis5467100% (1)
- DRUG STUDY (Erythromycin)Document3 pagesDRUG STUDY (Erythromycin)Avianna CalliopeNo ratings yet
- Azure Arc DoccumentDocument143 pagesAzure Arc Doccumentg.jithendarNo ratings yet