You might also like
- Genetic Counselling: Understanding RisksDocument6 pagesGenetic Counselling: Understanding RisksJanet VargheseNo ratings yet
- 1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Document54 pages1.1, 1.2, 1.3, 1.5 Paediatric Nursing Presentation - 1-1Christina YounasNo ratings yet
- A Study To Assess The Knowledge and Attitude of Postnatal Mother Regarding Postnatal Diet in A View of Developing Booklet at Selected Community AreaDocument14 pagesA Study To Assess The Knowledge and Attitude of Postnatal Mother Regarding Postnatal Diet in A View of Developing Booklet at Selected Community AreaIJAR JOURNALNo ratings yet
- Dissertation Presentation: REG - NO.19N02102035 Obstetrics and Gynecological NursingDocument62 pagesDissertation Presentation: REG - NO.19N02102035 Obstetrics and Gynecological NursingSanju Sudha100% (1)
- Genetic Patterns of Common Pediatric DisordersDocument29 pagesGenetic Patterns of Common Pediatric DisordersramNo ratings yet
- Failure to Thrive TeachingDocument10 pagesFailure to Thrive TeachingSAYMABANUNo ratings yet
- A Study To Assess The Knowledge of Mothers Regarding Weaning Among Children 6 Months To 2 Years of Age in Selected Rural Areas of Punjab IndiaDocument3 pagesA Study To Assess The Knowledge of Mothers Regarding Weaning Among Children 6 Months To 2 Years of Age in Selected Rural Areas of Punjab IndiaIJARP PublicationsNo ratings yet
- PLACENTA CLINICAL ASSESSMENT GUIDEDocument18 pagesPLACENTA CLINICAL ASSESSMENT GUIDEAbi RajanNo ratings yet
- Prevalence of Anemia Among Adolescent Girls in IndiaDocument6 pagesPrevalence of Anemia Among Adolescent Girls in IndiaYolanda SimamoraNo ratings yet
- Case Presentation SurgeryDocument9 pagesCase Presentation SurgeryFlora LawrenceNo ratings yet
- Birth Injuries: By: Murad Sawalha RN, MSNDocument18 pagesBirth Injuries: By: Murad Sawalha RN, MSNPriyanka JainNo ratings yet
- Teaching Method AssignmentDocument16 pagesTeaching Method AssignmentDivine HunuNo ratings yet
- Minor Discomfort and Complication Puerperium Topic FINALDocument14 pagesMinor Discomfort and Complication Puerperium Topic FINALsuman guptaNo ratings yet
- Nursing Assignment on Hemorrhage and Shock PathophysiologyDocument22 pagesNursing Assignment on Hemorrhage and Shock PathophysiologyaparnaNo ratings yet
- Child Health Nursing-I - 201022Document8 pagesChild Health Nursing-I - 201022ShwetaNo ratings yet
- Pap Smear - Overview, Indications, PreparationDocument11 pagesPap Smear - Overview, Indications, PreparationBayu Surya DanaNo ratings yet
- Ppt-Journal ClubDocument50 pagesPpt-Journal Clubgao1989No ratings yet
- Communicable DiseasesDocument56 pagesCommunicable DiseasesLili Nini100% (1)
- PHILOSOPHY of EducationDocument2 pagesPHILOSOPHY of EducationJisna AlbyNo ratings yet
- Unit VII Assessment of The Pediatric ClientDocument36 pagesUnit VII Assessment of The Pediatric ClientSyed Maaz100% (1)
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Annotated Bibliography: INTRODUCTION-An Annotated Bibliography Is Typically Short (Usually ADocument6 pagesAnnotated Bibliography: INTRODUCTION-An Annotated Bibliography Is Typically Short (Usually AVinita TiwariNo ratings yet
- 05 N001 40088Document23 pages05 N001 40088hariharad sourabhNo ratings yet
- Key Concepts MediaDocument20 pagesKey Concepts MediaaparnaNo ratings yet
- Ethical Issues in NeonateDocument11 pagesEthical Issues in Neonatethilaga880% (1)
- CERVICAL SMEAR SKILL LABDocument5 pagesCERVICAL SMEAR SKILL LABMuthiana Rizky0% (1)
- Trail of LaborDocument5 pagesTrail of LaborNithiya NadesanNo ratings yet
- Play is the work of childDocument57 pagesPlay is the work of childdeepika kushwahNo ratings yet
- My ThesisDocument46 pagesMy ThesisManish SharmaNo ratings yet
- Effect of A Training Program About Maternal Fetal Attachment Skills On Prenatal Attachment Among Primigravida WomenDocument6 pagesEffect of A Training Program About Maternal Fetal Attachment Skills On Prenatal Attachment Among Primigravida WomenInternational Organization of Scientific Research (IOSR)No ratings yet
- Ambiguous Genitalia Diagnosis and ManagementDocument8 pagesAmbiguous Genitalia Diagnosis and ManagementnasibdinNo ratings yet
- Research in Continuing Education Seminar Typed ContentDocument31 pagesResearch in Continuing Education Seminar Typed Contentpravina praviNo ratings yet
- Govt. College of Nursing, Siddhpur Subject: Obstetrics Nursing Topic: High Risk PregnancyDocument36 pagesGovt. College of Nursing, Siddhpur Subject: Obstetrics Nursing Topic: High Risk PregnancyJOSHI MITALINo ratings yet
- Theory Application in Nursing Practice-RevisedDocument17 pagesTheory Application in Nursing Practice-RevisedChandrashekar GajulaNo ratings yet
- Developmental Milestone of Preschool AgeDocument3 pagesDevelopmental Milestone of Preschool AgeJessa Mae BacuganNo ratings yet
- Club FootDocument24 pagesClub FootBhawna Pandhu100% (1)
- Ministry of Health and Family Welfare Pregnancy GuidelinesDocument173 pagesMinistry of Health and Family Welfare Pregnancy GuidelinesKhushi GuptaNo ratings yet
- Topic - Version Subject - ObgDocument23 pagesTopic - Version Subject - ObgMandeep KaurNo ratings yet
- Current StatusDocument14 pagesCurrent Statusthilaga88No ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadNo ratings yet
- Original Article A Study To Assess The Effectiveness of Planned Teaching ProgrammeDocument3 pagesOriginal Article A Study To Assess The Effectiveness of Planned Teaching ProgrammeAaliyaan KhanNo ratings yet
- Vancouver Style Referencing SystemDocument20 pagesVancouver Style Referencing SystemKarthik ManoharanNo ratings yet
- Factors Influencing LearningDocument17 pagesFactors Influencing Learningnirajan shresthaNo ratings yet
- High Risk Antenatal AssessmentDocument15 pagesHigh Risk Antenatal AssessmentAbishaNo ratings yet
- CLINICSDocument24 pagesCLINICSsonali mewarNo ratings yet
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDocument31 pagesNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNo ratings yet
- Postmature Infants 1Document13 pagesPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Intrauterine Growth RestrictionDocument27 pagesIntrauterine Growth RestrictionJorge La Serna InfantesNo ratings yet
- Newborn Osce Checklist: A. For StudentsDocument2 pagesNewborn Osce Checklist: A. For Studentsshubham vermaNo ratings yet
- Role of Midwifery NurseDocument6 pagesRole of Midwifery NurseLokeshwari KatreNo ratings yet
- LegalaspectsDocument47 pagesLegalaspectssanthiyasandy100% (1)
- Neonatal JaundiceDocument36 pagesNeonatal JaundiceJenaffer Achamma JohnNo ratings yet
- To Assess The Knowledge On Prevention and Control of Worm Infestations Among The Mothers' of Underfive Children at Erode, TamilnaduDocument3 pagesTo Assess The Knowledge On Prevention and Control of Worm Infestations Among The Mothers' of Underfive Children at Erode, TamilnaduInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nursing AuditDocument5 pagesNursing AuditGAGANJOT850% (1)
- Artificial Insemination GuideDocument3 pagesArtificial Insemination Guidesagi muNo ratings yet
- Nutrition essentials for pregnancyDocument33 pagesNutrition essentials for pregnancyNorman AjxNo ratings yet
- Patient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDocument93 pagesPatient Scenario, Chapter 45, Nursing Care of A Family When A Child Has A Gastrointestinal DisorderDay MedsNo ratings yet
- Low Amniotic Fluid LevelsDocument2 pagesLow Amniotic Fluid LevelspramaNo ratings yet
- IEC Role Health ServicesDocument70 pagesIEC Role Health ServicesAparna Aby100% (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Evaluation of Health ServicesDocument42 pagesEvaluation of Health Servicesdrsanjeev15No ratings yet
- Introduction of Med GeneticsDocument94 pagesIntroduction of Med Geneticsdrsanjeev15No ratings yet
- Classical Theories of PersonalityDocument29 pagesClassical Theories of PersonalityGunjanNo ratings yet
- Evaluation of Health ServicesDocument42 pagesEvaluation of Health Servicesdrsanjeev15No ratings yet
- Research Methodology Bio Statistics NetDocument100 pagesResearch Methodology Bio Statistics Netdrsanjeev15No ratings yet
- Primary Health Care in IndiaDocument37 pagesPrimary Health Care in Indiadrsanjeev15No ratings yet
- Introductory Lecture On Environment and Health: Dr. Sanjeev GuptaDocument20 pagesIntroductory Lecture On Environment and Health: Dr. Sanjeev Guptadrsanjeev15No ratings yet
- Dr. Sanjeev GuptaDocument73 pagesDr. Sanjeev Guptadrsanjeev15No ratings yet
- Strong Letter of Recommendation for Radiology ResidencyDocument1 pageStrong Letter of Recommendation for Radiology Residencydrsanjeev15No ratings yet
- Statistician's ChecklistDocument2 pagesStatistician's Checklistdrsanjeev15No ratings yet
- Guitar Chord Chart For Drop D TuningDocument4 pagesGuitar Chord Chart For Drop D TuningJnewsletter1No ratings yet
- The BarographDocument8 pagesThe BarographNazre ShahbazNo ratings yet
- MTSC QuestionsDocument8 pagesMTSC QuestionsAbhi RamNo ratings yet
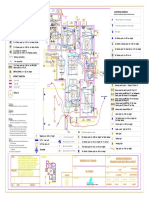
- Varun Valanjeri Electrical Layout-3Document1 pageVarun Valanjeri Electrical Layout-3ANOOP R NAIRNo ratings yet
- IEC 61850 Configuration of A Phoenix Contact IED: User ManualDocument68 pagesIEC 61850 Configuration of A Phoenix Contact IED: User ManualHarold PuinNo ratings yet
- Sales Confirmation: Alpha Trading S.P.A. Compagnie Tunisienne de NavigationDocument1 pageSales Confirmation: Alpha Trading S.P.A. Compagnie Tunisienne de NavigationimedNo ratings yet
- Refunds Maceda Law and PD957Document2 pagesRefunds Maceda Law and PD957QUINTO CRISTINA MAENo ratings yet
- (1902) The Centennial of The United States Military Academy at West Point New YorkDocument454 pages(1902) The Centennial of The United States Military Academy at West Point New YorkHerbert Hillary Booker 2nd100% (1)
- Remove Head IsmDocument67 pagesRemove Head IsmjeremyNo ratings yet
- Sat Psat Word GamesDocument166 pagesSat Psat Word Gamesapi-360773187No ratings yet
- Change Management HRDocument2 pagesChange Management HRahmedaliNo ratings yet
- Step 5 - PragmaticsDocument7 pagesStep 5 - PragmaticsRomario García UrbinaNo ratings yet
- Lab Skill Workbook - Applied Physics - Seph0009 07-12-2023Document87 pagesLab Skill Workbook - Applied Physics - Seph0009 07-12-2023rahulsaitalasilaNo ratings yet
- Edge Computing As A Service: How Macrometa is Revolutionizing Global Data ProcessingDocument8 pagesEdge Computing As A Service: How Macrometa is Revolutionizing Global Data ProcessingAtlantis-ILIONo ratings yet
- Route StructureDocument3 pagesRoute StructureAndrei Gideon ReyesNo ratings yet
- Administrator Guide: Document Version 3.6.1Document76 pagesAdministrator Guide: Document Version 3.6.1App PackNo ratings yet
- English Club ConstitutionDocument27 pagesEnglish Club ConstitutionJude Martin AlvarezNo ratings yet
- Business Studies Project: Made By: Rahil JainDocument29 pagesBusiness Studies Project: Made By: Rahil JainChirag KothariNo ratings yet
- Birla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionDocument5 pagesBirla Institute of Technology and Science, Pilani: Pilani Campus AUGS/ AGSR DivisionDeep PandyaNo ratings yet
- Kantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1Document13 pagesKantar Worldpanel Division FMCG Monitor Q2 2022 EN Including Gift Shared-by-WorldLine-Technology-1K59 Dau Minh VyNo ratings yet
- ICT4D - Richard Heeks (2305843009216382716)Document307 pagesICT4D - Richard Heeks (2305843009216382716)Jeff GeoffNo ratings yet
- The Coffee House-Group 8Document18 pagesThe Coffee House-Group 8Thanh Huyền TrầnNo ratings yet
- Pink Illustrative Weather Quiz Game PresentationDocument28 pagesPink Illustrative Weather Quiz Game PresentationMark Laurenze MangaNo ratings yet
- Wonder Woman: Directed byDocument4 pagesWonder Woman: Directed byRoxana Ioana DumitruNo ratings yet
- Solutions Manual To Accompany A Second Course in Statistics Regression Analysis 7th Edition 0321691695Document23 pagesSolutions Manual To Accompany A Second Course in Statistics Regression Analysis 7th Edition 0321691695DonnaLopezysned100% (36)
- THE HOUSE ON ZAPOTE STREET - Lyka PalerDocument11 pagesTHE HOUSE ON ZAPOTE STREET - Lyka PalerDivine Lyka Ordiz PalerNo ratings yet
- FVNL"'" - TT - ..: MycotaDocument8 pagesFVNL"'" - TT - ..: MycotaAmbesh JhaNo ratings yet
- Device Test ModeDocument14 pagesDevice Test ModeNay SoeNo ratings yet
- 35th Bar Council of India Moot Court MemorialDocument17 pages35th Bar Council of India Moot Court MemorialHarshit Mangal100% (3)
- Oracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentDocument4 pagesOracle Analytics Cloud 2018 Solution Engineer Specialist AssessmentRamón MedinaNo ratings yet