You might also like
- Pneumo PeritoneumDocument31 pagesPneumo PeritoneumRaif RizqullahNo ratings yet
- PneumoperitoneumDocument31 pagesPneumoperitoneumRaif RizqullahNo ratings yet
- RectumDocument129 pagesRectumRadhika SethuNo ratings yet
- Lap Chole Case StudyDocument3 pagesLap Chole Case StudyKinshuki Jain100% (1)
- Respiratory Diagnostic Tests & Procedures.Document32 pagesRespiratory Diagnostic Tests & Procedures.Salman KhanNo ratings yet
- Upper Gastrointestinal Endoscopy in Turkey: A Review of 5,000 CasesDocument2 pagesUpper Gastrointestinal Endoscopy in Turkey: A Review of 5,000 CasesEnderson MedeirosNo ratings yet
- Linear Atelectasis (Fig. 4.3) : Normally It Resolves Wiu1In Days or Weeks, But May Persist For LongerDocument90 pagesLinear Atelectasis (Fig. 4.3) : Normally It Resolves Wiu1In Days or Weeks, But May Persist For LongerMohammad Amin HosseiniNo ratings yet
- Case Report: Perforated Duodenal Diverticulum With Subtle Pneumoretroperitoneum On Abdominal X-RayDocument4 pagesCase Report: Perforated Duodenal Diverticulum With Subtle Pneumoretroperitoneum On Abdominal X-RayNoviaRiadyNo ratings yet
- PneumoperitoneumDocument15 pagesPneumoperitoneumMuhammad Dimas PangestuNo ratings yet
- Diagnostic Tests: 1-Pulmonary Function Tests (PFTS)Document13 pagesDiagnostic Tests: 1-Pulmonary Function Tests (PFTS)yuddNo ratings yet
- Laryngomalacia - PPTX Dr. FeriDocument114 pagesLaryngomalacia - PPTX Dr. FeriAldy BimaNo ratings yet
- Abnormal Bowel Gas PatternDocument136 pagesAbnormal Bowel Gas PatternEdward ElricNo ratings yet
- Pneumo PeritoneumDocument35 pagesPneumo PeritoneumDepinNo ratings yet
- Corpus Alienum PneumothoraxDocument3 pagesCorpus Alienum PneumothoraxPratita Jati PermatasariNo ratings yet
- Pinto 2016Document7 pagesPinto 2016Adinda ShafiraNo ratings yet
- Focused Assessment With Sonography For Trauma (Fast) and Extended-FastDocument49 pagesFocused Assessment With Sonography For Trauma (Fast) and Extended-FastajNo ratings yet
- Pathognomonic Imaging Signs in Abdominal RadiologyDocument11 pagesPathognomonic Imaging Signs in Abdominal RadiologyifzarNo ratings yet
- Jurnal Gastro PerforationDocument6 pagesJurnal Gastro PerforationYuke PutriNo ratings yet
- Radiografi AbdomenDocument55 pagesRadiografi AbdomenadikNo ratings yet
- Respiratory Distress Syndrome (HMD) MODocument77 pagesRespiratory Distress Syndrome (HMD) MOikhsan_drNo ratings yet
- Radio EmergencyDocument46 pagesRadio EmergencyRenz Mervin RiveraNo ratings yet
- Cystogram With Dumbbell Shaped Urinary Bladder in A Sliding Inguinal HerniaDocument12 pagesCystogram With Dumbbell Shaped Urinary Bladder in A Sliding Inguinal Hernia6281326189433No ratings yet
- Pediatric Imaging 2020Document84 pagesPediatric Imaging 2020shellers24No ratings yet
- Jurnal Diagnosa PneumoperitoniumDocument5 pagesJurnal Diagnosa PneumoperitoniumMustafa HolidiNo ratings yet
- Jurnal Radiologi NadiaDocument46 pagesJurnal Radiologi NadiaNadia Rezky ElizaNo ratings yet
- Jurding English FIXDocument24 pagesJurding English FIXDias Amardeka Putri GavintaNo ratings yet
- Post OperativeDocument54 pagesPost OperativeAli D Parsa100% (1)
- Chest TraumaDocument27 pagesChest TraumaGeraldine Marie SalvoNo ratings yet
- Ldcu Group 4 Buscaino April ShineDocument57 pagesLdcu Group 4 Buscaino April ShineApril Shine BuscainoNo ratings yet
- Imperforate AnusDocument52 pagesImperforate Anushayssam rashwan100% (6)
- ThoracentesisDocument21 pagesThoracentesisAmna BatoolNo ratings yet
- Fast Scan 2022Document9 pagesFast Scan 2022rosieNo ratings yet
- Paratracheal Abscess WLNDocument35 pagesParatracheal Abscess WLNYunita WulandariNo ratings yet
- ENT Approach To StridorDocument2 pagesENT Approach To StridorVanessa HermioneNo ratings yet
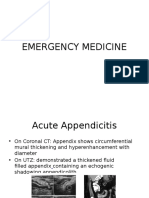
- Acute Appendicitis of The Appendiceal StumpDocument3 pagesAcute Appendicitis of The Appendiceal StumpXavier JarrínNo ratings yet
- Abdomen BOF 3Document78 pagesAbdomen BOF 3BakingpancakesNo ratings yet
- Tuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionDocument3 pagesTuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionwulanNo ratings yet
- X RaysDocument49 pagesX Rayskeithan96No ratings yet
- BautistajournDocument3 pagesBautistajournbomcorNo ratings yet
- Perforated Ileal Diverticulitis: CT Findings: İsmail Kırbaş, Erkan Yıldırım, Ali Harman, Özgür BaşaranDocument2 pagesPerforated Ileal Diverticulitis: CT Findings: İsmail Kırbaş, Erkan Yıldırım, Ali Harman, Özgür BaşaranKelfin ForceNo ratings yet
- Radiographic Signs of Gastrointestinal Perforation in Children: A Pictorial ReviewDocument8 pagesRadiographic Signs of Gastrointestinal Perforation in Children: A Pictorial ReviewMaria NatashaNo ratings yet
- EsophagosDocument18 pagesEsophagosHumra ShamimNo ratings yet
- Management of Tracheostimized Patients.Document33 pagesManagement of Tracheostimized Patients.Umaima KhanNo ratings yet
- Peritonsillar Abscess in Emergency MedicineDocument14 pagesPeritonsillar Abscess in Emergency Medicinerissa neNo ratings yet
- Perforasi EsofagusDocument4 pagesPerforasi EsofagusIcan DoitNo ratings yet
- Enarm Train Quiz AnswDocument284 pagesEnarm Train Quiz AnswanndreaoliveraNo ratings yet
- Laryngeal: Obstruction Relieved by PantingDocument3 pagesLaryngeal: Obstruction Relieved by PantingIndah D. RahmahNo ratings yet
- Ent Throat 1Document58 pagesEnt Throat 1ميمونه عبدالرحيم مصطفىNo ratings yet
- Trichobezoar With Large Bowel Obstruction in Children - Case ReportDocument3 pagesTrichobezoar With Large Bowel Obstruction in Children - Case ReportSajag GuptaNo ratings yet
- What Is Ultrasound?Document15 pagesWhat Is Ultrasound?Al-Mukashfi TahaNo ratings yet
- 013504-Frkovic PDFDocument6 pages013504-Frkovic PDFMuhamad Chairul SyahNo ratings yet
- Ultrasound Abdominal Alternative Peritoneal Lavage: J. Chambers & PilbrowDocument8 pagesUltrasound Abdominal Alternative Peritoneal Lavage: J. Chambers & PilbrowZuni TriyantiNo ratings yet
- Ruptured Hepatic Abscess Mimicking Perforated ViscusDocument3 pagesRuptured Hepatic Abscess Mimicking Perforated ViscusMichu VuNo ratings yet
- Jurnal 3Document5 pagesJurnal 3Caesar RiefdiNo ratings yet
- Role of Radiology in Acute AbdomenDocument37 pagesRole of Radiology in Acute AbdomenAli TahirNo ratings yet
- Effects of Laryngeal Cancer On VoiceDocument10 pagesEffects of Laryngeal Cancer On VoiceSanNo ratings yet
- AXR PresentationDocument30 pagesAXR PresentationLalit KumarNo ratings yet
- 1 s2.0 S1526820920302652 MainDocument8 pages1 s2.0 S1526820920302652 MainTogar gultomNo ratings yet
- CHT Hcfa Boys Z 0 13 9098091092309Document1 pageCHT Hcfa Boys Z 0 13 9098091092309neutralmindNo ratings yet
- Pocket Book of Hospital Care For ChildrenDocument438 pagesPocket Book of Hospital Care For ChildrenTawangNo ratings yet
- IMW025.04 Immunoglobulin Handbook Diphtheria Butana March2021Document9 pagesIMW025.04 Immunoglobulin Handbook Diphtheria Butana March2021Togar gultomNo ratings yet
- WHO Operational Protocols Diphtheria PDFDocument25 pagesWHO Operational Protocols Diphtheria PDFAnonymous hETtEBkk7No ratings yet
- Keira Knightley: Jump To Navigation Jump To SearchDocument12 pagesKeira Knightley: Jump To Navigation Jump To SearchCrina LupuNo ratings yet
- Sharp Product-Catalogue 2019 enDocument48 pagesSharp Product-Catalogue 2019 enMiki di KaprioNo ratings yet
- Project Proposal DraftDocument1 pageProject Proposal DraftCarl Axel M. FajardoNo ratings yet
- CA-idms Ads Alive User Guide 15.0Document142 pagesCA-idms Ads Alive User Guide 15.0svdonthaNo ratings yet
- Introduction To Physiotherapy PracticeDocument22 pagesIntroduction To Physiotherapy PracticejNo ratings yet
- Sample Engagement LetterDocument5 pagesSample Engagement Letterprincess_camarilloNo ratings yet
- Data Analyst Chapter 3Document20 pagesData Analyst Chapter 3Andi Annisa DianputriNo ratings yet
- Et200sp Im 155 6 PN ST Manual en-US en-USDocument47 pagesEt200sp Im 155 6 PN ST Manual en-US en-USayaz officeNo ratings yet
- Technical Assistance Plan School Year 2020-2021 Prioritized Needs of The Clients Objectives Strategies Activities MOV Time-Frame ResourcesDocument3 pagesTechnical Assistance Plan School Year 2020-2021 Prioritized Needs of The Clients Objectives Strategies Activities MOV Time-Frame ResourcesDon Angelo De Guzman95% (19)
- VRF Mv6R: Heat Recovery Outdoor UnitsDocument10 pagesVRF Mv6R: Heat Recovery Outdoor UnitsTony NguyenNo ratings yet
- E Commerce and Its Influence in Changing in Purchasing Behavior of Modern ConsumersDocument13 pagesE Commerce and Its Influence in Changing in Purchasing Behavior of Modern ConsumersRichard VillanuevaNo ratings yet
- Damask: by ChenoneDocument17 pagesDamask: by ChenoneYasir IjazNo ratings yet
- Chapter 7odeDocument29 pagesChapter 7odeRoberto NascimentoNo ratings yet
- A Dessertation Report Submitted in Partial Fulfillment of Requirements For The Award of The Degree ofDocument65 pagesA Dessertation Report Submitted in Partial Fulfillment of Requirements For The Award of The Degree ofMadhavpokale100% (1)
- Game On Series BibleDocument28 pagesGame On Series Bibleapi-513832615No ratings yet
- Trend Trading StocksDocument64 pagesTrend Trading Stockssasi717100% (1)
- FE 208 Lab #4 - Profile Leveling: CrewDocument4 pagesFE 208 Lab #4 - Profile Leveling: CrewJefferson Himson0% (1)
- Ken Holt 06 The Secret of Hangman's InnDocument216 pagesKen Holt 06 The Secret of Hangman's InnPastPresentFuture100% (2)
- Introductions and Basic Personal Information (In/Formal Communication)Document6 pagesIntroductions and Basic Personal Information (In/Formal Communication)juan morenoNo ratings yet
- HBS - Zara Fast Fashion Case Write UpDocument4 pagesHBS - Zara Fast Fashion Case Write Upaaronhwalton100% (1)
- AMX Prodigy Install ManualDocument13 pagesAMX Prodigy Install Manualsundevil2010usa4605No ratings yet
- Program Logic FormulationDocument69 pagesProgram Logic FormulationIan OffemariaNo ratings yet
- Quizlet Table 7Document1 pageQuizlet Table 7JosielynNo ratings yet
- AC AMMETER / Moving Iron: Model AECDocument33 pagesAC AMMETER / Moving Iron: Model AECRoonar Aponte NoaNo ratings yet
- PD750-01 Engine Data Sheet 12-29-20Document4 pagesPD750-01 Engine Data Sheet 12-29-20Service Brags & Hayes, Inc.No ratings yet
- Hotel Voucher: Itinerary ID Hotel Santika Taman Mini Indonesia IndahDocument2 pagesHotel Voucher: Itinerary ID Hotel Santika Taman Mini Indonesia IndahSyukron PribadiNo ratings yet
- Hydrogen ReviewDocument53 pagesHydrogen Reviewjuric98No ratings yet
- CV Old NicDocument4 pagesCV Old NicTensonNo ratings yet
- Bell Single-Sleeve Shrug Crochet PatternDocument2 pagesBell Single-Sleeve Shrug Crochet PatternsicksoxNo ratings yet
- Piezoelectric-Material Based Energy Harvesting Device.Document29 pagesPiezoelectric-Material Based Energy Harvesting Device.jobert100% (1)