You might also like
- Manual for the Implementation of Environmental, Health, and Safety Standards for the Control of Locusts: December 2021From EverandManual for the Implementation of Environmental, Health, and Safety Standards for the Control of Locusts: December 2021No ratings yet
- Bio-Medical Waste ManagementDocument25 pagesBio-Medical Waste ManagementmahendranNo ratings yet
- Effective microbiological sampling of food processing environments (1999)From EverandEffective microbiological sampling of food processing environments (1999)No ratings yet
- Bio Medical WasteDocument2 pagesBio Medical Wastesandeep AhujaNo ratings yet
- Bio-Medical Waste Rules GuideDocument19 pagesBio-Medical Waste Rules GuideAruna ChezhianNo ratings yet
- HAAD Policy On Medical WasteDocument10 pagesHAAD Policy On Medical WasteibrahimkhansahilNo ratings yet
- BIOMEDICAL WASTE REGULATIONS AND MANAGEMENTDocument21 pagesBIOMEDICAL WASTE REGULATIONS AND MANAGEMENTDrShweta SainiNo ratings yet
- BM Waste MGMT Issues Challenges040609Document23 pagesBM Waste MGMT Issues Challenges040609Nayan RoychowdhuryNo ratings yet
- BMW NewDocument63 pagesBMW NewHarshaWakodkarNo ratings yet
- Mitraj Health LawDocument4 pagesMitraj Health Lawmitraj parmarNo ratings yet
- Salient Features and Key Changes of Hazardous WasteDocument8 pagesSalient Features and Key Changes of Hazardous WasteKaladorNo ratings yet
- BM Waste Color CodingDocument23 pagesBM Waste Color Codingpriyankamote100% (1)
- 879 Chapter 64e-16 Biomedical WasteDocument9 pages879 Chapter 64e-16 Biomedical WasteMarkbot1999No ratings yet
- EL&ADocument15 pagesEL&ABhargav DaveNo ratings yet
- Bio-Medical Waste Management: With Specific Reference To RML Hospital, New DelhiDocument24 pagesBio-Medical Waste Management: With Specific Reference To RML Hospital, New DelhiUtpal RahaNo ratings yet
- BioMedical Waste Management Issues ChallengesDocument23 pagesBioMedical Waste Management Issues ChallengesArun Shree RNo ratings yet
- Bio Medical RulesDocument23 pagesBio Medical RulesSanjana GaneshNo ratings yet
- UntitledDocument59 pagesUntitledSakshi YadavNo ratings yet
- Bio-Medical Waste Management RulesDocument4 pagesBio-Medical Waste Management RulesSameer BaswanaNo ratings yet
- BMW ManagementDocument4 pagesBMW ManagementPramod SahNo ratings yet
- Bio-Medical Waste Rules SummaryDocument3 pagesBio-Medical Waste Rules SummaryRithik VisuNo ratings yet
- DENR - Proper Handling of Hazardous WasteDocument16 pagesDENR - Proper Handling of Hazardous WasteNisha HernandezNo ratings yet
- Daily News Simplified - DNS: SL. NO. Topics The Hindu Page NoDocument11 pagesDaily News Simplified - DNS: SL. NO. Topics The Hindu Page NoPrakul GuptaNo ratings yet
- 217_ Hospital Waste ManagementDocument31 pages217_ Hospital Waste Managementkhushi.gupta2122No ratings yet
- Laws Relating to Processing of Biomedical WasteDocument16 pagesLaws Relating to Processing of Biomedical WasteShalini SonkarNo ratings yet
- HTTP CDN - Cseindia.org Attachments 0.83054200 1601045646 Managing-biomedical-waste-In-India-reportDocument28 pagesHTTP CDN - Cseindia.org Attachments 0.83054200 1601045646 Managing-biomedical-waste-In-India-reportCH064PATEL RUDRANo ratings yet
- Biomedical Waste Management...... DR Sana Kauser PathologyDocument19 pagesBiomedical Waste Management...... DR Sana Kauser PathologyDr saleem Ahmed Abdul RasheedNo ratings yet
- Unit 6 Biomedical Waste ManagementDocument14 pagesUnit 6 Biomedical Waste ManagementjyothiNo ratings yet
- Biomedical Waste Management Guidelines - CompressedDocument60 pagesBiomedical Waste Management Guidelines - Compressedomkarsonawane517No ratings yet
- Presented By: J.G Sambad Ikdrc College of NursingDocument48 pagesPresented By: J.G Sambad Ikdrc College of Nursingshubham vermaNo ratings yet
- Env. Prot Act 1986 and Bio Medical WasteDocument3 pagesEnv. Prot Act 1986 and Bio Medical WastePandurang BagateNo ratings yet
- Biomedical Waste (Management & Handling) Rules 1998 Amended On 2000Document6 pagesBiomedical Waste (Management & Handling) Rules 1998 Amended On 2000hamid_hinnaNo ratings yet
- 1 Biomed Rules 1998Document15 pages1 Biomed Rules 1998livingd121No ratings yet
- Podiatry Waste ProtocolDocument8 pagesPodiatry Waste ProtocolmurraymedicalNo ratings yet
- Dr. Nguyen Thi Lien Huong Deputy Director, Vietnam Health Environment Management Agency, MOHDocument25 pagesDr. Nguyen Thi Lien Huong Deputy Director, Vietnam Health Environment Management Agency, MOHHealth Care Without Harm - AsiaNo ratings yet
- BMW-GUIDELINES-COVID - 2 - CPCB - Rev.05 - Apr 2022Document12 pagesBMW-GUIDELINES-COVID - 2 - CPCB - Rev.05 - Apr 2022Khyati PatelNo ratings yet
- Impact Analysis of The Bio-Medical Waste Management Through The Corona Virus PanDocument14 pagesImpact Analysis of The Bio-Medical Waste Management Through The Corona Virus PanAayush SinhaNo ratings yet
- Bio-Medical Waste Management (BMWM) Rules, 2016Document2 pagesBio-Medical Waste Management (BMWM) Rules, 2016hiteshNo ratings yet
- Biomedical Waste ManagmentDocument18 pagesBiomedical Waste ManagmentStephen MooreNo ratings yet
- TVP - Title - Concept - Description - : STORY: - One Fine Morning Mr. Thomas (Social Worker) in HisDocument7 pagesTVP - Title - Concept - Description - : STORY: - One Fine Morning Mr. Thomas (Social Worker) in HisLakshmanan SreenivasanNo ratings yet
- BMW rules salient featuresDocument2 pagesBMW rules salient featuresakankshaNo ratings yet
- BMW 1Document6 pagesBMW 1Nisha SinghNo ratings yet
- Who BMW SharpsDocument5 pagesWho BMW SharpsDrShruthi PradeepNo ratings yet
- Biomedical Waste Management Gujarat Pollution Control Board GandhinagarDocument35 pagesBiomedical Waste Management Gujarat Pollution Control Board GandhinagarDrVishal BhattNo ratings yet
- Project For Biomedical Waste Management at District Hospital and Medical College LevelDocument36 pagesProject For Biomedical Waste Management at District Hospital and Medical College LevelmikkijainNo ratings yet
- Bio-Medical Waste Management Rules: DR NaveenDocument26 pagesBio-Medical Waste Management Rules: DR Naveenmani kandanNo ratings yet
- Waste Management in HamidiyaDocument37 pagesWaste Management in Hamidiyavidhya associateNo ratings yet
- Adb Heal Code of Construction PracticeDocument27 pagesAdb Heal Code of Construction PracticeCris Jan BanaagNo ratings yet
- Guidelines for Handling Biomedical WasteDocument6 pagesGuidelines for Handling Biomedical WasteShubhra ShastriNo ratings yet
- Bio Medical Waste DisposalDocument10 pagesBio Medical Waste DisposalShanender Singh SambyalNo ratings yet
- Guidelines For Management of Bio-Medical Waste Contaminated / Suspected To Be Contaminated With COVID-19Document3 pagesGuidelines For Management of Bio-Medical Waste Contaminated / Suspected To Be Contaminated With COVID-19Indranil MitraNo ratings yet
- Hospital Waste Management Laws and RealitiesDocument40 pagesHospital Waste Management Laws and RealitiesYogesh ChandraNo ratings yet
- Compliance RCO ConditionsDocument2 pagesCompliance RCO ConditionsprastacharNo ratings yet
- Central Govt. rules for environmentally sound management of biomedical wasteDocument17 pagesCentral Govt. rules for environmentally sound management of biomedical wastepriscila_macwanNo ratings yet
- Bio Medical Waste Rules in IndiaDocument6 pagesBio Medical Waste Rules in IndiaPandurang BagateNo ratings yet
- Bio-Medical Waste Management: Issues and ChallengesDocument74 pagesBio-Medical Waste Management: Issues and ChallengesKarthick VNo ratings yet
- Bio-Medical Waste Management 02Document16 pagesBio-Medical Waste Management 02ravsab GaikwadNo ratings yet
- dm2021-0405 IPCDocument6 pagesdm2021-0405 IPCLearsi AfableNo ratings yet
- Biomedical Waste Management Rules SummaryDocument30 pagesBiomedical Waste Management Rules SummaryAshish TiwariNo ratings yet
- Hospital Waste Plan OptimizedDocument37 pagesHospital Waste Plan OptimizedDarren Cariño100% (3)
- Unit 1 QuestionsDocument1 pageUnit 1 QuestionsRithisha JaganNo ratings yet
- UNIT 1 - Lecture 8 - Role of M, L, MDocument51 pagesUNIT 1 - Lecture 8 - Role of M, L, MRithisha JaganNo ratings yet
- UNIT 1 Lecture 7 TelemedicineDocument33 pagesUNIT 1 Lecture 7 TelemedicineRithisha JaganNo ratings yet
- Cardiac PressureDocument9 pagesCardiac PressureRithisha JaganNo ratings yet
- PBF Energy Response To CEC November 29th Hearing InvitationDocument5 pagesPBF Energy Response To CEC November 29th Hearing InvitationRob NikolewskiNo ratings yet
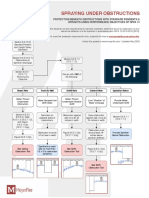
- Sprinkler Obstruction CheatsheetDocument1 pageSprinkler Obstruction CheatsheetKarkare89100% (1)
- Termites Syn SDSDocument6 pagesTermites Syn SDSafiq.npcNo ratings yet
- Final Project Writeup AM+KW 20100506Document9 pagesFinal Project Writeup AM+KW 20100506Kyle Wayne WilliamsNo ratings yet
- APA Brochure 2019-Kk830-Updated 9.3Document34 pagesAPA Brochure 2019-Kk830-Updated 9.3Farhad TavassoliNo ratings yet
- Budj Bim Cultural LandscapeDocument7 pagesBudj Bim Cultural LandscapeArchi PrajapatiNo ratings yet
- Soil fauna and food webs as indicators of agro-ecosystem disturbanceDocument9 pagesSoil fauna and food webs as indicators of agro-ecosystem disturbanceFábio Luís MostassoNo ratings yet
- Landfill Gas Energy Project Development Handbook (EPA)Document143 pagesLandfill Gas Energy Project Development Handbook (EPA)ChrisMurilloNo ratings yet
- Wireless Turbidity Sensor Node Using PIC16F877A and X-Bee: P.M.Gavhane, P.P. Tadwalkar, V. D. Bachuwar, D.S.SutraveDocument3 pagesWireless Turbidity Sensor Node Using PIC16F877A and X-Bee: P.M.Gavhane, P.P. Tadwalkar, V. D. Bachuwar, D.S.SutraveSou TVNo ratings yet
- EcoKids project promotes environmental awarenessDocument11 pagesEcoKids project promotes environmental awarenessJosphine Mundava MaringaNo ratings yet
- Simapro ExerciseDocument2 pagesSimapro Exerciseburty1No ratings yet
- Siphonic Roof Drainage Systems ExplainedDocument7 pagesSiphonic Roof Drainage Systems ExplainedRenzo Marquina AstoNo ratings yet
- Rainforest Alliance Sustainable Agriculture Standard: Farm RequirementsDocument89 pagesRainforest Alliance Sustainable Agriculture Standard: Farm RequirementsKaye UntalanNo ratings yet
- Janapriya Journal of Interdisciplinary Studies - Vol - 6Document186 pagesJanapriya Journal of Interdisciplinary Studies - Vol - 6abiskarNo ratings yet
- 3-A Accepted Practice For Plant Environmental Air Quality, Number 612-00Document12 pages3-A Accepted Practice For Plant Environmental Air Quality, Number 612-00CHRISTIAN ZAVALANo ratings yet
- Dissertation On Sustainable HousingDocument8 pagesDissertation On Sustainable HousingSomeoneToWriteMyPaperGlendale50% (2)
- AMB 172-024 Forklift OperationsDocument2 pagesAMB 172-024 Forklift OperationsRues AgNo ratings yet
- SGLGB AwardingDocument12 pagesSGLGB AwardingRonz RoganNo ratings yet
- Penerapan Pola Pertanian Vertikal (Larian) Di Lahan Pegunungan Oleh Masyarakat Suku Tengger Dalam Perspektif Hukum LingkunganDocument25 pagesPenerapan Pola Pertanian Vertikal (Larian) Di Lahan Pegunungan Oleh Masyarakat Suku Tengger Dalam Perspektif Hukum Lingkunganputri muziraNo ratings yet
- Human Environment SystemDocument23 pagesHuman Environment Systemangelo zeus fernandezNo ratings yet
- Waste Not Want Not Useful WorksheetsDocument13 pagesWaste Not Want Not Useful WorksheetsBestil AyNo ratings yet
- Example 1 - Reflection ReportDocument10 pagesExample 1 - Reflection ReportILYA IZATIENo ratings yet
- DEDR Hupsekot, Final PDFDocument75 pagesDEDR Hupsekot, Final PDFAmul ShresthaNo ratings yet
- World War-II Wreck Diving To Palawan PhilippinesDocument6 pagesWorld War-II Wreck Diving To Palawan PhilippinesLisaNo ratings yet
- NSTP Waste ManagementDocument6 pagesNSTP Waste ManagementIrish Sophia OlimpoNo ratings yet
- Cities and Municipalities in CARAGA Region with Tourist AttractionsDocument8 pagesCities and Municipalities in CARAGA Region with Tourist AttractionsRoselyn AcbangNo ratings yet
- Marketing Management Chapter 2Document33 pagesMarketing Management Chapter 2Mohammed KumashNo ratings yet
- Kuhn Archimedean ScrewsDocument2 pagesKuhn Archimedean ScrewsitovarsilvaNo ratings yet
- 0016 K1fkc5kubDocument6 pages0016 K1fkc5kubNandar Min HtetNo ratings yet
- Frutee GMB3L User GuideDocument1 pageFrutee GMB3L User GuidexyzNo ratings yet