You might also like
- Mazda 6 2014 - Automatic Transaxle Workshop Manual FW6A-EL PDFDocument405 pagesMazda 6 2014 - Automatic Transaxle Workshop Manual FW6A-EL PDFFelipe CalleNo ratings yet
- Upper Limb OrthosisDocument83 pagesUpper Limb OrthosisAwaisNo ratings yet
- Orthotics 121208142340 Phpapp01Document94 pagesOrthotics 121208142340 Phpapp01Raghu Nadh100% (1)
- Powerful and Durable JCB JS200 Tracked ExcavatorDocument6 pagesPowerful and Durable JCB JS200 Tracked ExcavatorMB Viorel100% (1)
- ArthroplastyDocument64 pagesArthroplastyAmit Kochhar75% (4)
- KAFO and KO Guide for Lower Limb StabilizationDocument35 pagesKAFO and KO Guide for Lower Limb StabilizationMaryam KhalidNo ratings yet
- Improving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsFrom EverandImproving Ankle and Knee Joint Stability: Proprioceptive Balancefit Discs DrillsNo ratings yet
- Battle Bikes 2.4 PDFDocument56 pagesBattle Bikes 2.4 PDFfranzyland100% (1)
- Lower Extremity ProsthesisDocument148 pagesLower Extremity ProsthesisDanielle Louise Caingat100% (1)
- OrthosisDocument112 pagesOrthosisChandan MahapatraNo ratings yet
- Ortho Instruments & ImplantsDocument106 pagesOrtho Instruments & ImplantsBi PinNo ratings yet
- Prosthesis: Presented by Dr. Chiranjeevi.JDocument63 pagesProsthesis: Presented by Dr. Chiranjeevi.JchirusdunnaNo ratings yet
- Guidelines For Selecting Materials For Downhole Completions Equipment (Jewellery)Document32 pagesGuidelines For Selecting Materials For Downhole Completions Equipment (Jewellery)Slim.BNo ratings yet
- Lower Extremity Orthosis: Noel R. San Antonio, PTRP MSCPDDocument27 pagesLower Extremity Orthosis: Noel R. San Antonio, PTRP MSCPDLeo LopezNo ratings yet
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- OYO Case Study SolutionDocument4 pagesOYO Case Study SolutionVIKASH GARGNo ratings yet
- 5G Antenna Talk TWDocument48 pages5G Antenna Talk TWRohit MathurNo ratings yet
- Orthosis 130814094004 Phpapp02Document23 pagesOrthosis 130814094004 Phpapp02Anisha KhanalNo ratings yet
- KAFODocument34 pagesKAFOBedo GikryNo ratings yet
- Sapamine CSN Textile Softener: Technical Data SheetDocument5 pagesSapamine CSN Textile Softener: Technical Data SheetsaskoNo ratings yet
- Philippine Orthopedic Center Lecture NotesDocument7 pagesPhilippine Orthopedic Center Lecture Notesxteovisio100% (2)
- Lower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyDocument56 pagesLower Limb Orthosis: Dr. Sumit Raghav, PT Assistant Professor Jyotirao Subharti College of PhysiotherapyKavya Mittal100% (2)
- Goethe Zertifikat b1 HorenDocument2 pagesGoethe Zertifikat b1 HorenLevent75% (4)
- Selecting Running Shoes: Injury Prevention and Performance EnhancementDocument21 pagesSelecting Running Shoes: Injury Prevention and Performance EnhancementSagar DeshpandeNo ratings yet
- OrthosisDocument35 pagesOrthosissinghmenkaNo ratings yet
- Foot Orthosis and Lower Limb Bracing GuideDocument25 pagesFoot Orthosis and Lower Limb Bracing GuideAbdul Al-FattahNo ratings yet
- RRASSINGMENTDocument12 pagesRRASSINGMENTAditi RajoraNo ratings yet
- ORTHOTIC BASICSDocument94 pagesORTHOTIC BASICSAkbar AziziNo ratings yet
- Prosthetics and Orthotics SHS.424: DR Asma WadoodDocument41 pagesProsthetics and Orthotics SHS.424: DR Asma WadoodMina JavedNo ratings yet
- AFO and Shoe Modifs (1)Document58 pagesAFO and Shoe Modifs (1)sanika pradhanNo ratings yet
- Knee and Hip OrthosisDocument4 pagesKnee and Hip Orthosis楊畯凱No ratings yet
- Calipers - Lower ExtremityDocument40 pagesCalipers - Lower ExtremityNivetha RavikumarNo ratings yet
- MOC Notes 2011 NewDocument181 pagesMOC Notes 2011 NewMohit GuptaNo ratings yet
- Ankle Foot OrthosesDocument14 pagesAnkle Foot OrthosesRohail Farid OrakzaiNo ratings yet
- Prosthetic Foot Characteristics: Lecture Four Artificial Organs 1 Dr. Waleed JasimDocument12 pagesProsthetic Foot Characteristics: Lecture Four Artificial Organs 1 Dr. Waleed Jasimزهراء حيدر ميريNo ratings yet
- OrthothicsDocument32 pagesOrthothicsRafael Miguel MallillinNo ratings yet
- introduction to bioengineeringDocument35 pagesintroduction to bioengineeringsanika pradhanNo ratings yet
- Orthotics Course Objectives and TerminologyDocument19 pagesOrthotics Course Objectives and TerminologyKanwal KhanNo ratings yet
- Protetika StopalaDocument37 pagesProtetika StopalaAmar TupkusicNo ratings yet
- Evaluation Procedures For Lower Limb OrthosesDocument19 pagesEvaluation Procedures For Lower Limb OrthosesMaryam KhalidNo ratings yet
- Artificial LimbDocument51 pagesArtificial LimbBhaskar Borgohain100% (2)
- GAYO - Activity 1 Week 2 OPATDocument5 pagesGAYO - Activity 1 Week 2 OPATart gayoNo ratings yet
- Orthosis and ProsthesisDocument25 pagesOrthosis and Prosthesissanika pradhanNo ratings yet
- Prosthesis GuideDocument14 pagesProsthesis GuideUganeswary Venugopal100% (1)
- ProsthesisDocument23 pagesProsthesisdoc-fahad aftabNo ratings yet
- Lower Extremity Orthotics - 2023 - SVDocument86 pagesLower Extremity Orthotics - 2023 - SVashlyn granthamNo ratings yet
- Orthosis AGA Dan SpinalDocument57 pagesOrthosis AGA Dan SpinalJuwita KusumadewiNo ratings yet
- Evolution of Artificial LimbsDocument51 pagesEvolution of Artificial LimbsNada GhammemNo ratings yet
- Hip Guidance OrthosisDocument2 pagesHip Guidance OrthosisSangeetha GnaneswaranNo ratings yet
- EVIDENCE-BASED MANAGEMENT OF PLANTAR FASCIITISDocument40 pagesEVIDENCE-BASED MANAGEMENT OF PLANTAR FASCIITISMohamed ElMeligieNo ratings yet
- AFO Design and ComponentsDocument18 pagesAFO Design and ComponentsNafisah Bochil100% (1)
- Prosthesis: Uganeswary VenugopalDocument14 pagesProsthesis: Uganeswary VenugopalUganeswary VenugopalNo ratings yet
- Microprocessor Knee UnitsDocument54 pagesMicroprocessor Knee UnitsKumar BalramNo ratings yet
- Presented By: DR Venkatesh V Moderator: DR Harish KDocument81 pagesPresented By: DR Venkatesh V Moderator: DR Harish KPankaj VatsaNo ratings yet
- Artrocare Cti 2: Additional EquipmentDocument7 pagesArtrocare Cti 2: Additional EquipmentIonela PascarNo ratings yet
- Prosthesis (Lower Limb) 20207221046560Document22 pagesProsthesis (Lower Limb) 20207221046560Kavya Mittal100% (1)
- Exercise Science Isu Pictures TablesDocument7 pagesExercise Science Isu Pictures Tablesapi-282118209No ratings yet
- OrtesisDocument15 pagesOrtesisTito IglesiasNo ratings yet
- AFO Design and Components: Understanding Ankle Foot OrthosesDocument18 pagesAFO Design and Components: Understanding Ankle Foot Orthosesdilla fifiani nurhalifahNo ratings yet
- Below Knee Prosthesis and Components: Reported By: DELA, Angelica Joy A. MAGALING, JuliusDocument33 pagesBelow Knee Prosthesis and Components: Reported By: DELA, Angelica Joy A. MAGALING, JuliusDenise De la CruzNo ratings yet
- Or Tho TicsDocument11 pagesOr Tho TicsvsripathirajaNo ratings yet
- BFO - Review of Pathology KAFODocument6 pagesBFO - Review of Pathology KAFOnovitaNo ratings yet
- Knee Joint Functions and Knee Orthosis TypesDocument40 pagesKnee Joint Functions and Knee Orthosis TypesAlfred JacksonNo ratings yet
- Range of Motion Guide for Physical TherapistsDocument2 pagesRange of Motion Guide for Physical TherapistsGERALD ZAMORACAPERANo ratings yet
- 09 AfoDocument107 pages09 AfonovitaNo ratings yet
- 08 Endo - Model - Standaard - M - Mireto - Imp - Amp - Instr - 03 - 2020Document52 pages08 Endo - Model - Standaard - M - Mireto - Imp - Amp - Instr - 03 - 2020Daniela Carvallo BarriosNo ratings yet
- Alimusaj 2009 Kinematics and Kinetics With An AdaDocument8 pagesAlimusaj 2009 Kinematics and Kinetics With An AdaAlioune Badara DioufNo ratings yet
- ds923 Virtex Ultrascale PlusDocument81 pagesds923 Virtex Ultrascale Plusismail topcuNo ratings yet
- Economics Principles and Policy 13th Edition Baumol Solutions ManualDocument2 pagesEconomics Principles and Policy 13th Edition Baumol Solutions ManualCraigGonzalezaxzgd100% (17)
- String inverter comparisonDocument4 pagesString inverter comparisonRakesh HateyNo ratings yet
- BCG ReportDocument9 pagesBCG Reportjlgjlj ljglkhNo ratings yet
- Developing Website Information ArchitectureDocument39 pagesDeveloping Website Information ArchitectureBizuNo ratings yet
- Research 10 Mod2Document28 pagesResearch 10 Mod2Fernadez RodisonNo ratings yet
- AllareDocument16 pagesAllareGyaniNo ratings yet
- Segmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Document2 pagesSegmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Boon-Pin NgNo ratings yet
- Overview of Research ProcessDocument31 pagesOverview of Research Processprema balusamyNo ratings yet
- Reaction Order and Rate Law Expression Worksheet KeyDocument5 pagesReaction Order and Rate Law Expression Worksheet KeyLyra GurimbaoNo ratings yet
- Kütahya between the Lines: Uncovering Historical Insights from Post-Medieval CeramicsDocument24 pagesKütahya between the Lines: Uncovering Historical Insights from Post-Medieval Ceramicslatinist1No ratings yet
- Modigliani MillerDocument12 pagesModigliani MillerAlvaro CamañoNo ratings yet
- Group ActDocument3 pagesGroup ActRey Visitacion MolinaNo ratings yet
- My Demo DemoDocument19 pagesMy Demo DemoAlex LopezNo ratings yet
- Material 01 - Human-Computer InteractionDocument8 pagesMaterial 01 - Human-Computer InteractionIlangmi NutolangNo ratings yet
- Band Theory and Bloch Theorem in Solid State PhysicsDocument8 pagesBand Theory and Bloch Theorem in Solid State PhysicsVicky VickyNo ratings yet
- OlayDocument36 pagesOlayrachit.chaudharyNo ratings yet
- PTR01 21050 90inst PDFDocument40 pagesPTR01 21050 90inst PDFЯн ПавловецNo ratings yet
- Results and DiscussionsDocument13 pagesResults and DiscussionsEdpher Leo SindolNo ratings yet
- Strategic Marketing Plan for British American TobaccoDocument31 pagesStrategic Marketing Plan for British American TobaccoAli Abbas50% (2)
- Agile Spotify - Team - HomeworkDocument8 pagesAgile Spotify - Team - Homeworksp76rjm7dhNo ratings yet
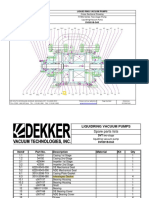
- Bomba de Vacio Part ListDocument2 pagesBomba de Vacio Part ListNayeli Zarate MNo ratings yet